Download

1 / 39
600 likes | 1.97k Views
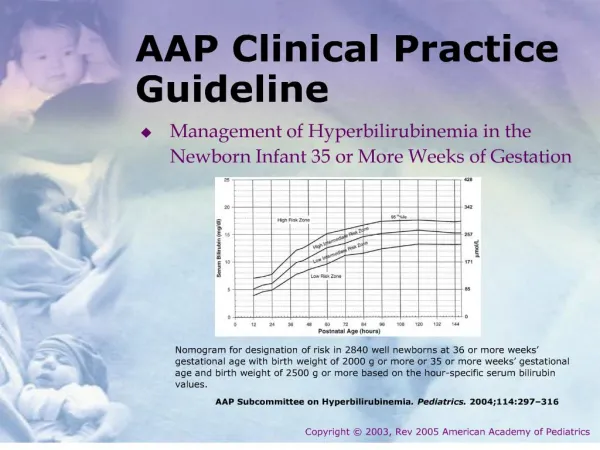
AAP Clinical Practice Guidelines Bronchiolitis. Dominic C. Sia, M.D. Bronchiolitis. characterized by acute inflammation edema and necrosis of epithelial cells lining small airways increased mucus production bronchospasm.

E N D
AAPClinical Practice GuidelinesBronchiolitis Dominic C. Sia, M.D.
Bronchiolitis • characterized by • acute inflammation • edema and necrosis of epithelial cells lining small airways • increased mucus production • bronchospasm • a disorder most commonly caused in infants by viral lower respiratory tract infection (LRTI). • the most common lower respiratory infection in children 1 month – 2 years of age
Signs and Symptoms • rhinitis • tachypnea • wheezing • cough • Crackles • nasal flaring • use of accessory muscles
RSV • Most common etiologic agent for bronchiolitis • highest incidence of infection occurring between December and March • 90% of children infected within first 2 years of life • up to 40% of them will have lower respiratory infection • Infection with RSV does not grant permanent or long-term immunity • Reinfections are common
RSV • RSV infection leads to more than 90000 hospitalizations annually • Mortality has decreased • 4500 deaths annually in 1985 in US • estimated 510 in 1997 and 390 in 1999 • cost of hospitalization for bronchiolitis in children <1 yr old estimated to be >$700M/yr
Other Agents Bronchiolitis • human metapneumovirus • influenza • adenovirus • parainfluenza
Post Infection • Children who present with severe disease • persistently increased respiratory effort • apnea, • need for intravenous hydration, supplemental oxygen, or mechanical ventilation are more likely to present with respiratory problems as older children (recurrent wheezing)
AAP Guidelines • 1 month – 2 years of age • Excluding children with immunodeficiencies or underlying chronic lung or heart disease • Grading • A-B Strong Recommendation • B-C Recommendation • D Optional • X Strong recommendation
Guideline 1 Recommended • Diagnosis should be made clinically, without routine use of laboratory or radiologic tests • Assessment should risk factors for severe disease • Prematurity • underlying lung or heart disease • immunodeficiency
Guideline 1 Recommended • infants presenting with cough and/or wheeze, particularly in the winter season • differentiation of infants with probable bronchiolitis from those with other disorders • estimation of the severity of illness • tachypnea • 50 breaths per minute in term newborns • 40 breaths per minute at 6 months of age • 30 breaths per minute at 12 months
Guideline 1 Recommended • Important issues to assess • impact of respiratory symptoms on feeding and hydration • response, if any, to therapy • ability of the family to care for the child and return for further care • may require serial observations over time
Guideline 1 Recommended • Risk Factors for Severity • premature birth (less than 37 weeks) • young age of the child (less than 6–12 weeks) • Development of apneic episodes • hemodynamically significant congenital heart disease • chronic lung disease (BPD, Cystic Fibrosis, etc • presence of an immunocompromised state • tachypnea, defined as a respiratory rate of 70 or more
Guideline 1 Recommended • Pulse oximetry • small correlation between oximetry and risk of prolonged hospitalization, ICU admission, and mechanical ventilation • Chest DX • current evidence does not support routine radiography in children with bronchiolitis
Guideline 1 Recommended • CBC • Risk of SBIs very low • has not been shown to be useful in either diagnosing bronchiolitis or guiding its therapy • Virologic testing • rarely alters management decisions or outcomes • virologic testing may be useful when cohorting of patients
Guideline 2 Recommended • Bronchodilators should not be used routinely for management • Optional trial of ß-agonist should be continued only if objective evaluation indicates a clinical response • Most studies show transient improvement of unclear clinical significance
Guideline 2 Recommended • albuterol or nebulized epinephrine had no significant effect on duration of illness or length of hospital stay • Epinephrine > Albuterol • office or clinic setting - use albuterol/salbutamol • document pretherapy and posttherapy changes using an objective means of evaluation
Guideline 2 Recommended • documented clinical improvement continue the nebulized bronchodilator • in the absence of a clinical response, the treatment should not be continued • no justification for use of anticholinergic agents with or without ß-adrenergic agents • insufficient data regarding use of leukotriene modifiers
Guideline 3 Recommended • Routine use of corticosteroids is not recommended • no improvement found in • respiratory rate • Hb oxygen saturation • hospital revisit • hospital readmission rates
Guideline 4 Recommended • Routine use of ribavirin is not recommended
Guideline 4 Recommended • marginal benefit • cumbersome delivery requirements • potential health risks for caregivers • high cost • may be considered for use in highly selected situations • severe disease • immunocompromised • hemodynamically significant cardiopulmonary disease
Guideline 5 Recommended • Antibiotics should be used only when bacterial infection is clearly present
Guideline 5 Recommended • low rates of SBI (0%–3.7%) • more likely to be a UTI than bacteremia or meningitis • ~ 25% of hospitalized infants will have radiographic evidence of atelectasis or infiltrates, often misinterpreted as SBI • Bacterial pneumonia in infants with bronchiolitis without consolidation is unusual • 50-75% with AOM • 95% with isolates Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis • AOM did not influence the clinical course • AOM should be managed according to the AAP/AAFP guidelines
Guideline 6Strongly Recommended • Assessment of hydration status and oral intake should be done regularly • Treatment with intravenous fluids is recommended if necessary
Guideline 6Strongly Recommended • When RR 60 to 70 or > feeding may be compromised • nasal secretions are copious • increased risk of aspiration of food into the lungs • NOTE: possibility of fluid retention related to production of antidiuretic hormone has been reported in patients with bronchiolitis
Guideline 7 Recommended • Routine chest physiotherapy is not recommended • No clinical benefit of using vibration and percussion techniques • Suctioning of the nares may provide temporary relief of nasal congestion • no evidence to support routine "deep" suctioning of the lower pharynx or larynx.
Guideline 8 Optional • Supplemental O2 and continuous monitoring are not routinely recommended unless Spo2 persistently <90% • oxygen should be used to maintain Spo2 at 90% or greater • infant’s clinical work of breathing may also be considered in the decision to use supplemental oxygen. • NOTE: Careful oxygen weaning in infants with prematurity or hemodynamically significant heart or lung disease.
Guideline 8 Optional • when SpO2 is above 90%, large increases in PaO2 are associated with small increases in SpO2 • when SpO2 is below 90%, a small decrease in PaO2 is associated with large decreases in SpO2 • factors including fever, acidosis, and some hemoglobinopathies shift the curve • Low SpO2 • repositioning the probe • Check nose and oral airway and suction if necessary
Guideline 9Strongly Recommended • Prophylactic palivizumab is recommended in selected high-risk children with prematurity or heart or lung disease • administered in 5 monthly doses during the respiratory syncytial virus (RSV) season (Nov-Mar) • Palivizumab’s benefits outweigh its costs
Guideline 9Strongly Recommended • 2006 Report of the Committee on Infectious Disease Red Book • <24 months of age with chronic lung disease of prematurity who have required medical therapy (supplemental oxygen, bronchodilator or diuretic or corticosteroid therapy) for CLD within 6 months before the start of the RSV season • Patients with more severe CLD who continue to require medical therapy may benefit from prophylaxis during a second RSV season • infants born at 29 to 32 weeks of gestation may benefit most from prophylaxis up to 6 months of age
Guideline 9Strongly Recommended • 2006 Report of the Committee on Infectious Disease Red Book • for infants born between 32 and 35 weeks of gestation prophylaxis should be reserved • <6 months of age at the start of the RSV season • child care attendance • school-aged siblings • exposure to environmental air pollutants • congenital abnormalities of the airways • severe neuromuscular disease
Guideline 10 Recommended • Hand washing is strongly recommended • Educate personnel and family members on hand hygiene • preferably with alcohol-based rubs or antimicrobial soaps • before and after contact with patient • contact with objects in patient’s vicinity • after removing gloves
Guideline 11 Recommended • Infants should not be exposed to passive smoking • Breast-feeding decreases the risk for RSV and other LRTI • threefold greater risk for nonbreastfed
Guideline 12 Optional • Asking parents about their use of complementary and alternative therapies is optional
Guideline 12 Optional • Complementary and Alternative Therapies (CAM) • Homeopathy • herbal remedies • osteopathic manipulation • applied kinesiology • 1 recent trial • herbal preparation containing Echinacea, propolis, and vitamin C • prevented the development of URI infections in children between the ages of 1 and 5 years.
Future Investigations • development of rapid, cost-effective tests for viruses other than RSV that may also play a role in bronchiolitis • studies to determine if there are selected patients who may benefit from bronchodilators or corticosteroids • clinical studies of the target SpO2 for the most efficient use of oxygen and oxygen monitoring • development of new therapies including new antiviral medications • continued research into the development of an RSV vaccine • continued development of immunoprophylaxis that would require fewer doses and decreased cost
Summary • Diagnosis should be made clinically, without routine use of laboratory or radiologic tests, and should include assessment of risk factors for severe disease (e.g., prematurity, underlying lung or heart disease, and immunodeficiency) • Bronchodilators should not be used routinely for management. An optional trial of an - or ß-agonist should be continued only if objective evaluation indicates a clinical response. • Routine use of corticosteroids is not recommended • Routine use of ribavirin is not recommended • Antibiotics should be used only when bacterial infection is clearly present • Assessment of hydration status and oral intake is strongly recommended. IV fluids should be given as necessary • Routine chest physiotherapy is not recommended
Summary • Supplemental O2 and continuous monitoring are not routinely recommended unless Spo2 persistently falls below 90%. The infant’s clinical work of breathing may also be used to determined need for supplemental oxygen • Prophylactic palivizumab is recommended in selected high-risk children with prematurity or heart or lung disease • Hand washing is strongly recommended, preferably with alcohol-based rubs or antimicrobial soaps • Infants should not be exposed to passive smoking and breast-feeding is recommended to decrease the risk for RSV and other LRTI • Asking parents about their use of complementary and alternative therapies is optional