Download
1 / 3

E N D
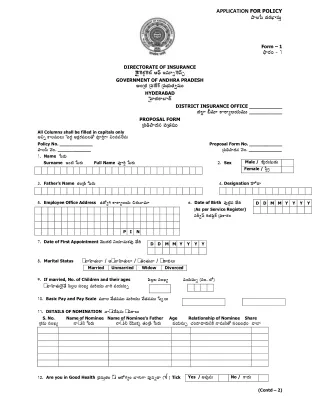
APPLICATION FOR POLICY FyÌÁ{qs µR¶LRiÆØxqsVò Form – 1 FnyLRiLi c 1 DIRECTORATE OF INSURANCE \®\®²¶lLiNíRPlLiÉÞ A£mns B©«sW=lLi©±s= GOVERNMENT OF ANDHRA PRADESH ALiúµ³R¶ úxms®µ¶[a`P úxms˳ÏÁV»R½*ª«sVV HYDERABAD \|¤¦¦¦µR¶LSËص`¶ DISTRICT INSURANCE OFFICE ___________ ÑÁÍýØ ÕdÁª«sW NSLSùÌÁ¸R¶Vª«sVV ___________ PROPOSAL FORM úxms¼½FyµR¶©«s xmsú»R½ª«sVV All Columns shall be filled in capitals only @¬sõ NSÌÁª«sVVÌÁV |msµôR¶ @ORPQLRiª«sVVÌÁ»][ xmspLjiògS ¬sLixmsª«sÛÍÁ©«sV Policy No. ___________ FyÌÁ{qs ®©sLi. ___________ 1. Name }msLRiV Surname BLiÉÓÁ }msLRiV 3. Father’s Name »R½Liú²T¶ }msLRiV 5. Employee Office Address Dµ][ùgjiNSLSùÌÁ¸R¶V ÀÁLRiV©yª«sW Proposal Form No. ___________ úxms¼½FyµR¶©«s ®©sLi. ___________ 2. Sex Female / {qsòQû Full Name xmspLjiò }msLRiV Male / xxxmsoLRiVxtsv²R¶V 4. Designation xx¤¦Ü[µy 6. Date of Birth xmsoÉíÓÁ©«s ¾»½[µj¶ (Asper Service Register) xqsLki*£qs LjiÑÁxtísQL`i úxmsNSLRiLi D D M M Y Y Y Y P I N 7. Date of First Appointment ®ªsVVµR¶ÉÓÁ ¬s¸R¶Wª«sVNRPxmso ¾»½[µj¶ 8. Marital Status - sªyz¤¦¦¦»R½VÍØ / @- sªyz¤¦¦¦»R½VÍØ / - s»R½Li»R½Vªy / - s²yNRPVÌÁV Married 9. If married, No. of Children and their ages zmsÌýÁÌÁ xqsLiÅÁù ª«s¸R¶VxqsV= (xqsLi. ÍÜ[) - sªyz¤¦¦¦»R½V\ÛÍÁ¾»½[ zmsÌýÁÌÁ xqsLiÅÁù ª«sVLji¸R¶VV ªyLji ª«s¸R¶VxqsV= 10. Basic Pay and Pay Scale ª«sVWÌÁ®ªs[»R½©«sª«sVV ª«sVLji¸R¶VV ®ªs[»R½©«sª«sVV }qsäÌÁV 11. DETAILS OF NOMINATION ©y- sV®©s[xtsQ©«sV - sª«sLSÌÁV S. No. Name of Nominee Name of Nominee’s Father Age Relationship of Nominee Share úNRPª«sV xqsLiÅÁù ©y- sV¬s }msLRiV ©y- sV¬s ¹¸¶VVNRPä »R½Liú²T¶ }msLRiV 12. Are you in Good Health úxmsxqsVò»R½Li - dsV AL][gRiùLi ËØgRiVgS ª«so©«sõµy ( ) Tick D D M M Y Y Y Y Unmarried Widow Divorced ª«s¸R¶VxqsV= ¿RÁLiµyµyLRiV¬sNTP ©yª«sV¬s»][ xqsLiÊÁLiµ³R¶Li ªyÉØ Yes / @ª«so©«sV No / NSµR¶V (Contd – 2)
:: 2 :: 13. Have you in the preceeding (3) years been absent on Leave on Medical Grounds for more than (10) days at a time ? If Yes, give details gRi»R½ ª«sVW²R¶V xqsLiª«s»R½=LSÌÁÍÜ[ - dsVLRiV \®ªsµR¶ù NSLRißØÌÁ \|ms IZNP[ryLji (10) L][ÇÁÙÌÁNRPV \|msgS |qsÌÁª«so \|ms \lgiLRiV¥¦¦¦ÇÁLRi¸R¶WùLS ? @LiVV¾»½[ A - sª«sLSÌÁV ¾»½ÌÁxmsLi²T¶ 14. 1. Have you ever suffered from any of the following Diseases :- C úNTPLiµj¶ }msL]ä©«sõ ªyùµ³R¶VÌÁÍÜ[ ®µ¶[¬s»][\®©s©y - dsVLRiV FsxmsöV\®²¶©y Ëص³R¶xms²ïyLS ? Fs. Heart Ailment gRiVLi®²¶ªyùµ³j¶ ÕÁ. Kidney zqs. Cancer ²T¶. Lungs 2. If Yes, give details of Disease, duration and Treatment received xqsª«sWµ³y©«sª«sVV @ª«so©«sV @LiVV©«s, ªyùµ³j¶ - sª«sLSÌÁV, ÀÁNTP»R½= ¼d½xqsVN]¬s©«s \®ªsµR¶ù }qsª«sÌÁ - sª«sLSÌÁV ¾»½ÌÁöLi²T¶ 15. Are you a physically challenged person. If so, enclose Certificate issued by a Competent Authority - dsVNRPV G\®µ¶©y aSLkiLRiNRP ÍÜ[xmsLigS¬s \®ªsNRPùÌÁLigS¬s D©«sõQÈýÁLiVV¾»½[ @ÉíÓÁ @LigRi\®ªsNRPÌÁùLi - sª«sLSÌÁV ¾»½ÌÁxmsLi²T¶, \®ªsµyùµ³j¶NSLji ÇØLki ¿Á[zqs©«s @LigRi\®ªsNRPÌÁùLi µ³R¶Xª«sxmsú»y¬sõ xqsª«sVLjiöLi¿RÁLi²T¶ 16. If already insured Bµj¶ª«sLRiZNP[ ÕdÁª«sW ¿Á[zqsD©«sõ¿][ FyÌÁ{qs ®©sLi. 17. Proposed Monthly Premium úxms¼½Fyµj¶LiÀÁ©«s®©sÌÁxqsLji ú{ms- sV¸R¶VLi 18. Month and Year of Recovery »R½gæjiLixmso ÇÁLjigji©«s ®©sÌÁ ª«sVLji¸R¶VV xqsLiª«s»R½=LRiLi 19. Mobile No. ®ªsVV\ÛËÁÍÞ ®©sLi. 20. Email Address B®ªsVVLiVVÍÞ ÀÁLRiV©yª«sW Yes / @ª«so©«sV No / NSµR¶V Yes / @ª«so©«sV No / NSµR¶V Yes / @ª«so©«sV No / NSµR¶V ª«sVWú»R½zmsLi²R¶Li Yes / @ª«so©«sV No / NSµR¶V NSù©«s=LRiV Yes / @ª«so©«sV No / NSµR¶V EzmsLji ¼½»R½VòÌÁV Yes / @ª«so©«sV No / NSµR¶V Policy No. Total Monthly Premium ®©sÌÁxqsLji ú{ms- sV¸R¶VL ®ªsVV»R½òLi 21. Aadhar Card No. Aµ³yL`i NSL`ïi ®©sLi. 22. Employee ID No. Dµ][ùgji gRiVLjiòLixmso ®©sLi. 23. Major Head |msµôR¶ xmsµôR¶V Try. D. D. O. Code úÛÉÁÇÁLki ²T¶. ²T¶. J. N][²`¶ úxms¼½FyµR¶NRPV¬s LRiW²³T¶ úxmsNRPÈÁ©«s Declaration by the Proponent úªyzqsLi\®µ¶©«s©«sV NSNRPF¡LiVV©«s©«sV úxms¼½ @LiaRPLi ¸R¶Vµ³yLóRiLi, xqsª«sVúgRiLi, xqsLixmspLñRiLi @LiVV©«sª«s¬s¸R¶VV G xmsLjizqós»R½VÌÁNRPV xqsLiÊÁLiµ³j¶LiÀÁ ®©s[©«sV xqsª«sW¿yLRiª«sVV @LiµR¶Â¿Á[¸R¶Vª«sÌÁzqs¸R¶VV©«sõµ][ A xmsLjizqós»R½VÌÁ©«sV ¬sÖÁzms®ªs[¸R¶VÛÍÁ[µR¶¬s¸R¶VV ÛÍÁ[µy LRix¤¦¦¦xqsùLigS ª«soLi¿RÁÛÍÁ[µR¶¬s¸R¶VV ®©s[©«sV BLiµR¶V ª«sVWÌÁª«sVVgS úxmsNRPÉÓÁLi¿RÁV¿RÁV©yõ©«sV. \|ms - sª«sLRißáÌÁV ª«sVLji¸R¶VV C úxmsNRPÈÁ©«s ÕdÁª«sW N]LRiNRPV úxms¼½Fyµj¶LiÀÁ©«s IxmsöLiµy¬sNTP úFy¼½xmsµj¶NRPÌÁVgS ª«soLi²yÌÁ¬s¸R¶VV ®©s[©«sV ÊÁVµôðj¶xmspLRi*NRPLigS, G\®µ¶©y xqs»R½ù µR¶WLRi\®ªsV©«s - sª«sLRißá©«sV ¿Á[zqs©«sÈýÁVgS¬s, ¾»½ÖÁ¸R¶VxmsLRi¿RÁª«sÌÁzqsª«so©«sõ G\®µ¶©y xmsLjizqós¼½¬s ®ªsWxqsxmso ÊÁVµôðj¶»][ µyÀÁ ª«soLiÀÁ©«sÈýÁVgS¬s, BLiµR¶V- dsVµR¶ÈÁ NRP©«sVg]©«sõ ¹¸¶V²R¶ÌÁ xqsµR¶LRiV NSLiúÉØNíRPV úNTPLiµR¶ ¿ÁÖýÁLiÀÁ¸R¶VV©«sõ ú{ms- sV¸R¶Vª«sVVÌÁ¬sõLiÉÓÁ¬s N][ÍÜ[öª«sÛÍÁ©«s¬s¸R¶VV, A IxmsöLiµR¶Li xqsLixmspLñRiLigS LRiµôR¶V NSª«sÌÁ©«s¬s¸R¶VV ®©s[©«sV IxmsöVN]©«sV¿RÁV©yõ©«sV." "úxmsaRPõÌÁ©«sV xmspLjigS @LóRiLi ¿Á[xqsVNRPV©«sõ »R½LS*»R½ ®©s[©«sV \|ms©«s ¾»½ÖÁzms©«s - sª«sLRiª«sVVÌÁV Bª«s*²R¶ª«sVLiVVLiµj¶. @- s ©yxqs*µR¶xqsWòLji»][ (Contd – 3)
:: 3 :: understanding the questions, the same are true, full and complete whether written in my own hand writing or not in every particular and that I have not withheld or concealed any circumstances with regard to which information has been required from me. I agree that the foregoing statements and declaration shall be the basis of the proposed contract for an Insurance and that if it shall hereafter appear that I have willfully made any untrue statement or have fraudulently concealed any circumstances which I ought to have made known then all the Premia which shall have been paid under the said contract shall be forfeited and the contract rendered absolutely null and void.” ¾»½[µj¶ Date úxms¼½FyµR¶©«s \|ms G @µ³j¶NSLji xqsª«sVORPQLiÍÜ[ xqsLi»R½NRPLi ¿Á[¸R¶VÊÁ²T¶©«sµ][ A @µ³j¶NSLji µ³R¶X- dsNRPLRißá xmsú»R½Li CERTIFIED BY OFFICER BEFORE WHOM THE PROPOSAL IS SIGNED \|ms©«s }msL]ä©«sõ xqsLki*xqsV - sª«sLSÌÁV xqsLji\¹¸¶V©«sª«s¬s¸R¶VV, úxms¼½FyµR¶NRPV²R¶V ©y xqsª«sVORPQLiÍÜ[ xqsLi»R½NRPLi ¿Á[zqs©y²R¶¬s¸R¶VV ®©s[©«sV µ³R¶Xª«sxmsLRiVxqsVò©«s©y©«sV. ©«sW»R½©«s / @µR¶©«sxmso ÕdÁª«sW ¬s- sV»R½òª«sVV »R½gæjiLixmso ¿Á[zqs©«s ®ªsVVµR¶ÉÓÁ ú{ms- sV¸R¶VLi LRiW. ________________ ª«sVLji¸R¶VV ®ªsVV»R½òª«sVV LRiW. ___________ (Bµj¶ ª«sLRiZNP[ »R½gæjiLixmso ¿Á[zqs©«s ª«sVLji¸R¶VV úxmsxqsVò»R½ ú{ms- sV¸R¶VLi NRPÌÁVxmsoN]¬s) ___________ ®©sÌÁ ª«sVLji¸R¶VV ___________ xqsLiª«s»R½=LRiª«sVV ®ªs[»R½©«sª«sVV ©«sVLi²T¶ ¾»½[µj¶ ___________ gRiÌÁ ÉÜ[NRP©±s ®©sLiÊÁLRiV ___________ µy*LS ª«sxqsWÌÁV ¿Á[¸R¶V²R¶ª«sVLiVV©«sµj¶. been affixed in my presence. The First Premium recovered for fresh /subsequent Insurance is all _____________ (including previous and present Premium) from the pay of _________________ month and _____________ year, vide token No. ____________ dated __________________ xqósÌÁLi Station ¾»½[µj¶ Date ForOFFFICE USE O.R. ( ) “I do hereby declare that the foregoing details and Answers have been given by me after fully ÒÁ- s»R½ ÕdÁª«sW ¿Á[¸R¶VµR¶ÌÁÀÁ©«s ª«sùQQNTPò xqsLi»R½NRPLi Signature I certify that the service particulars stated above are correct and the Proponent’s Signature has ___________ in Ax¤¦¦¦LRißá ª«sVLji¸R¶VV ÊÁÉØ*²R¶ @µ³j¶NSLji (Ax¤¦¦¦LRißá ª«sVLji¸R¶VV ÊÁÉØ*²R¶ @µ³j¶NSLji gRiÑÁÛÉÁ²`¶ NS¬s ¹¸¶V²R¶ÌÁ A \|ms gRiÑÁÛÉÁ²`¶ @µ³j¶NSLji xqsLi»R½NRPª«sVV ¿Á[¸R¶Vª«sÌÁ¸R¶VV©«sV. ª«sVLji¸R¶VV {qs*¸R¶V µ³R¶X- dsNRPLRißá ¿ÁÌýÁµR¶V.) xqsLi»R½NRPª«sVV Signature Drawing and Disbursing Officer (If DDO is not gazetted, it should be countersigned by next Gazetted Officer and Self Attestation is not acceptable) x¤¦Ü[µy Designation NSLSùÌÁ¸R¶V ª«sVVúµR¶ Office Seal Supdt. DIO Please visit our Website : www.apgli.ap.gov.in for further information and guidelines