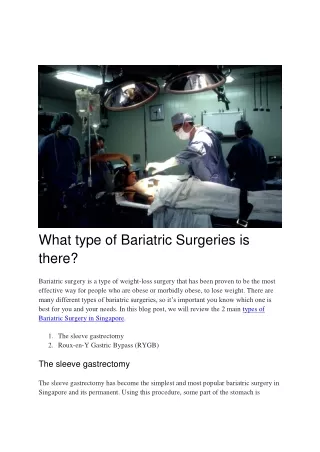
Weight Loss Surgery
While there are a number of non surgical diet plans available, bariatric surgery, whether itu2019s gastric bypass, lap band surgery or sleeve gastrectomy, produces the best results for achieving long-term success. Bariatric Surgery Can Effectively Treat Type 2 Diabetes, High Blood Pressure, and Sleep Apnea. Bariatric surgery has been documented as reducing premature death rates and improving, if not curing, the co-morbidities (other related illnesses) associated with being obese. Weu2019ve also seen improvement with arthritis general pain, mobility, asthma, infertility, and lymphedema. Dr. Terushkin deeply cares about his patients, their health and wellbeing, which is why he wants them to be successful. When it comes to choosing the right weight loss solution/program, he works directly with his patients and certified staff to come up with tailored individual plans for every case. This is done, so patients can loose weight, keep it off and implement the lifestyle changes necessary to stay healthy and live happy lives. Sleeve Gastrectomy. Sleeve Gastronomy is also known as gastric sleeve surgery, or u201csleeveu201d, procedure. During this procedure, the left side of the stomach is removed, leaving a stomach roughly the size and shape of a banana. Through 5 key-hole sized incisions, roughly 80% of the stomach is removed making patients feel full quicker and thus giving them better portion control. The segment of the stomach which is removed also houses hormone producing cells (Ghrelin- also known as a hunger hormone) which trigger hunger and therefore, once that portion of stomach is removed, hunger levels/cravings also tend to diminish. Sleeve gastrectomy also markedly improves most obesity-related comorbidities such as diabetes, sleep apnea, hypertension and hyperlipidemia.
52 views • 2 slides







![[Free Ebook] The Complete Bariatric Cookbook and Meal Plan Recipes and Guidance](https://cdn5.slideserve.com/11191243/free-ebook-the-complete-bariatric-cookbook-dt.jpg)


![[PDF]❤️DOWNLOAD⚡️ Bariatric Mindset Success: Live Your Best Life and Keep the Weight off After Weight Loss Surgery](https://cdn7.slideserve.com/12730783/slide1-dt.jpg)