Download
1 / 49
530 likes | 1.01k Views
The Oxford classification of IgA-nephropathy: A review based on the Polish renal biopsy registry . Agnieszka Perkowska-Ptasińska 1 , Małgorzata Węgrowska-Danilewicz, Marian Danilewicz, Agnieszka Hałoń, Anna Andrzejewska, Krzysztof Okoń, Henryk Karkoszka. 1 Medical University of Warsaw.

E N D
The Oxford classification of IgA-nephropathy: A review based on the Polish renal biopsy registry Agnieszka Perkowska-Ptasińska1, Małgorzata Węgrowska-Danilewicz, Marian Danilewicz, Agnieszka Hałoń, Anna Andrzejewska, Krzysztof Okoń, Henryk Karkoszka. 1Medical University of Warsaw
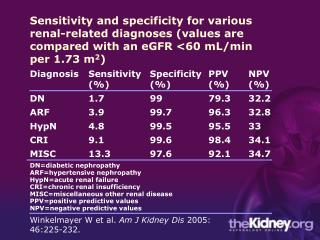
IgA nephropathy is the most common type of chronic glomerulonephritis in the world. • Up to 30% of clinically affected patients develop progressive renal failure, typically through a slow progression of CKD. • Non-specific clinical manifestation. • Diagnosis based on biopsy finding: the recognition of diffuse mesangial deposits of IgA in glomeruli. • Kidney biopsy is necessary to recognize IgA-N, but how much does it tell about the individual patient’s risk of kidneys insufficiency ?
Several studies devoted to the identification of histopathologic features that most accurately predict adverse outcome
In a majority of studies tubulointerstitial scarring was found to be an independent predictor of progression to ESRD in a multivariate analysis. • Glomerular lesions were usually found to correlate significantly with disease progression by univariate analysis, but rarely were they found to be independent predictors of such progression bya multivariate analysis. • The introduction of composite scoring systems (such as in Radford’s study) was associated with an enhancement of the negative predictive value of the glomerular lesions.
IgA-N histological grading according to the Joint Committee of the Research Group on Progressive Renal Disease and the Japanese Society of Nephrology (”the Japanese classification”, Wakai 2006)
Oxford classification of IgA-N The aim of the Oxford study: to develop a reproducible pathological classification of IgAN that would predict the clinical outcome. • Developed by renal pathologists and nephrologists from the international IgA nephropathy network and the RPS. • A study based on 265 patients with at least 1 year of follow-up. • Initially: selection of pathological variables that had high interobserver reproducibility and reliability. • Subsequently: identification of 4 pathological features which, independently of one another and of the patient’s clinical parameters, predicted the outcome. KI (2009) 76
The aim of the PHIGANS study • To discern the prognostic values of histological IgA-N characteristics defined by: Oxford, Haas, Japanese classifications, and PHIGANS – the Polish histological IgAnephropathy system).
Selection of IgA-N cases: dataset of the Polish Registry of Nephropathies Pathologists from the Polish nephropathological working group Agnieszka Perkowska-Ptasińska Małgorzata Danilewicz Marian Danilewicz Agnieszka Hałoń Anna Andrzejewska Krzysztof Okoń Henryk Karkoszka Nephrologists Ewa Komuda-Leszek Ilona Kurnatowska Monika Kraśnicka Tomasz Hryszko Mariusz Kusztal
PHIGANS STUDY Study design: retrospective Inclusion criteria: biopsy-proven IgA nephropathy recognized not later than in December 2008 with histological slides available for current re-evaluation, patients’ age >18 years, at least 12 months post-biopsy follow-up, clinical data available: - at the time of the biopsy - 3-6 months after the biopsy - 1 year after the biopsy - at the end of the observation
Clinical end points: Oxford study: • Rate of loss of renal function (ml/min/1.73 m2 per year), • ≥50% loss of renal function or ESRD (<15 ml/min/1.73 m2) by the end of the follow-up, Additional end point in PHIGANS study: 3. eGFR (MDRD) < 60 ml/min/1.73 m2by the end of the follow-up.
PHIGANS study - patients’ clinical characteristics at different time points
PHIGANS study: pharmaphological supportive treatment during the time of observation
PHIGANS study: pharmaphological treatment during the time of observation - immunosuppression
Results PHIGANS study Oxford study
54.7% 35% 0.9% 28.2% 16.2% 1% 35% 49% 57% 28% 16% 4% 22% Distribution of CKD stages among patients studied at the time of BX Oxford study (KI (2009) 76) PHIGANS study
frequency 60 80 -20 20 40 0 frequency 40 80 60 -20 0 20 Distribution of chronic lesions PHIGANS study:Mean number of glomeruli per biopsy: 21 ± 11.1 Oxford study:Mean number of glomeruli per biopsy: 18 Segmental GS KI (2009) 76: 534-545 Global GS
PHIGANS study 80 60 40 20 0 1-25% of cortex area with ci/ct no ci/ct frequency 26-50% of cortex area with ci/ct >50% of cortex area with ci/ct 0 1 2 3 60 in 1 - 25% of glomeruli 50 40 frequency 30 20 In 25 - 50% of glomeruli 10 In >50% of glomeruli 0 0 1 2 3 Distribution of chronic lesions Oxford study interstitial fibrosis/ tubular atrophy KI (2009) 76: 534-545 Fibrotic crescents
Japanese classification Haasclassification Frequency Frequency PHIGANS study: distribution of pathological grades according tothe Haas and Japanese classifications
Results of the statistical analysis • Correlations between the clinical parameters (at Bx) and histopathological variables defined according to the Oxford, Hass, Japanese, PHIGANS classifications. • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as eGFR<60 ml/min by the end of the observation (Cox regression analysis). • Relation between histopathological parameters and progression defined as eGFR loss≥20% by the end of the observation in pts with initial eGFR<60 ml/min (univariate analysis). • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as≥50% of eGFR loss or ESRD by the end of the observation (Cox regression analysis). • Relation between clinical (at Bx) as well as histopathological variables and the rate of GFR loss (dGFR) (linear regression).
Results of the statistical analysis • Correlations between the clinical parameters (at Bx) and histopathological variables defined according to the Oxford, Hass, Japanese, PHIGANS classifications. • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as eGFR<60 ml/min by the end of the observation (Cox regression analysis). • Relation between histolopathogical parameters and progression defined as eGFR loss≥20% by the end of the observation in pts with initial eGFR<60 ml/min (univariate analysis). • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as≥50% of eGFR loss or ESRD by the end of the observation (Cox regression analysis). • Relation between clinical (at Bx) as well as histopathological variables and the rate of GFR loss (dGFR) (linear regression).
Correlations between the clinical parameters (at Bx) and histopathological variables defined according to Oxford class. KI (2009) 76: 534-545
Correlations between the clinical parameters (at Bx) and histopathological variables according to PHIGANS
Correlations between the clinical parameters (at Bx) and histopathological variables according to PHIGANS
PHIGANS study: correlations between the clinical parameters (at Bx) and histopathological variables defined according to the Haas and Japanese classifications
Results of the statistical analysis • Correlations between the clinical parameters (at Bx) and histopathological variables defined according to the Oxford, Hass, Japanese, PHIGANS classifications. • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as eGFR<60 ml/min by the end of observation (Cox regression analysis). • Relation between the histopathological parameters and progression defined as eGFR loss≥20% by the end of observation in pts with initial eGFR<60 ml/min (univariate analysis). • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as≥50% of eGFR loss or ESRD by the end of the observation (Cox regression analysis). • Relation between the clinical (at Bx) as well as histopathological variables and the rate of GFR loss (dGFR) (linear regression).
Relation between the clinical variables (at Bx) and the outcome defined as eGFR<60 ml/min by the end of FU- univariate analysis
Relation between histopathological variables and the outcome defined as eGFR<60 ml/min by the end of FU- a univariate analysis
Cox regression model frequency OX-T GFR 16-69 GFR 70-94 vs 95-208 vs 95-208 Relation between the clinical (at Bx) as well as Oxfordhist. variables and the outcome defined as eGFR<60 mil/min by the end of FU-a multivariate analysis
Cox regression model HR Ct2 vs ct0 ct1 vs ct0 GFR 16-69 GFR 70-94 vs 95-208 vs 95-208 Relation between clinical (at Bx) as well as PHIGANS variables and the outcome defined as a eGFR<60 mil/min by the end of FU- a multivariate analysis
Results of the statistical analysis • Correlations between the clinical parameters (at Bx) and histopathological variables defined according to the Oxford, Hass, Japanese, PHIGANS classifications. • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as eGFR<60 ml/min by the end of observation (Cox regression analysis). • Relation between histopathological parameters and progression defined as eGFR loss≥20% by the end of the observation in pts with the initial eGFR<60 ml/min (univariate analysis). • Relation between the clinical (at Bx) as well as histopathological variables and the outcome defined as≥50% of eGFR loss or ESRD by the end of observation (Cox regression analysis). • Relation between the clinical (at Bx) as well as histopathological variables and the rate of GFR loss (dGFR) (linear regression).
OX-T: 0 1 (absent/present) OX-T: 0 1 2 Relation between histopathological parameters andprogression defined as eGFR loss≥20% by the end of the observation in pts with the initial eGFR<60 mil/min- a univariate analysis
ci: 0 1 2 3 GC st: 0 1 2 Relation between histopathological parameters and progression defined as eGFR loss≥20% by the end of the observation in pts with the initial eGFR<60 mil/min- a univariate analysis
Results of the statistical analysis • Correlations between the clinical parameters (at Bx) and histopathological variables defined according to the Oxford, Hass, Japanese, PHIGANS classifications. • Relation between clinical (at Bx) as well as histopathological variables and the outcome defined as eGFR<60 ml/min by the end of the observation (Cox regression analysis). • Relation between histopathological parameters and progression defined as eGFR loss≥20% by the end of the observation in pts with the initial eGFR<60 ml/min (univariate analysis). • Relation between clinical (at Bx) as well as histopathological variables and the outcome defined as≥50% of eGFR loss or ESRD by the end of observation (Cox regression analysis). • Relation between clinical (at Bx) as well as histopathological variables and the rate of GFR loss (dGFR) (linear regression).
Relation between the clinical (at Bx)as well as PHIGANS variables and the outcome defined as≥50% of eGFR loss or ESRD by the end of the observation- a univariate analysis
Cox regression model HR OX-T GFR 16-69 GFR 70-94 vs 95-208 vs 95-208 Relation between clinical (at Bx)and Oxford histopathological variables and the outcome defined as≥50% loss of eGFR or ESRD by the end of the observation - a multivariate analysis
Relation between Haas as well as Japanese classifications and the outcome – univariate analysis • In univariate analysis Cox regression analysis revealed an association between the 4th stage of the disease according to Japanese classification and an end point defined as GFR< 60 mil/min.
Results of the statistical analysis • Correlations between clinical parameters (at Bx) and histopathological variables defined according to Oxford, Hass, Japanese, PHIGANS classifications. • Relation between clinical (at Bx) as well as histopathological variables and the outcome defined as eGFR<60 ml/min by the end of observation (Cox regression analysis). • Relation between histopathological parameters and progression defined as eGFR loss≥20% by the end of observation in pts with initial eGFR<60 ml/min (univariate analysis). • Relation between clinical (at Bx) as well as histopathological variables and the outcome defined as≥50% of eGFR loss or ESRD by the end of observation (Cox regression analysis). • Relation between clinical (at Bx) as well as histopathological variables and the rate of GFR loss (dGFR) (linear regression).
Cellular crescents GFR at the time of Bx dGFR dGFR Relation between clinical parameters (at Bx)and the rate of GFR loss (dGFR) - linear regression, univariate analysis P=0.06 P<0.0001
IS therapy dGFR P=0.03 Relation between clinical parameters (at Bx) and the rate of GFR loss (dGFR) - linear regression, univariate analysis
Parameters in the best model (AIC: 782.48) with Haas classification p Haas classification 0.04 GFR <0.001 IS therapy 0.002 Relation between the activity/stage of the IgAN according to Haas class. and the rate of GFR loss (dGFR) - linear regression, multivariate analysis Haas classification dGFR P=0.04
Japanese classification Parameters in the best model (AIC: 787.8) with the Japanese classification p Japanese classification 0.02 dGFR GFR <0.001 IS therapy 0.004 Relation between the activity/stage of the IgAN according to Japanese classification and the rate of GFR loss (dGFR) - linear regression, multivariate analysis P=0.02
OX-T dGFR Relation between clinical as well as Oxford’s histop. variablesand the rate of GFR loss (dGFR) linear regression, multivariate analysis P=0.04
Biopsy index dGFR Relation between clinical as well as PHIGANSvariables and the rate of GFR loss (dGFR) linear regression, multivariate analysis P=0.002
Summary • eGFR at the time of Bx is the strongest clinical predictor of poor outcome in IgA nephropathy. • Among histopathological parameters defined by Oxford classification only tubular atrophy was found to be a negative prognostic factor in both univariate and multivartiate analysis with the end-point defined as eGFR <60 mil/min at the end of FU. • Among PHIGANS parameters the ones most distinctly associated with the clinical outcome were those that scored chronic lesions, with the strongest negative impact of tubulointerstitial scarring and composite scores, including biopsy index. Those scores have also correlated with the clinical manifestation of IgA at the time of biopsy (proteinuria and eGFR). • Japanese and Haas classifications were proved to have a significant negative impact on dGFR in the multivariate analysis.
Conclusions • The PHIGANS study has not confirmed the independent predictive value of glomerular lesions (segmentalsclerosis, mesangial and endocapillary hypercellularity) that was documented by the Oxford study. • The usage of composite scores makes the impact of glomerular lesions on the clinical outcome more distinct. • There were differences in both clinical and pathological characteristics of patients’ groups in PHIGANS and Oxford studies – to what extent have these differences caused the results’ discrepancies?