Download
1 / 41
430 likes | 974 Views
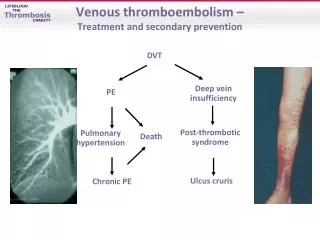
Prevention of Venous Thromboembolism Surgical Care Improvement Project. Dale W. Bratzler, DO, MPH President and CEO Oklahoma Foundation for Medical Quality. Dale W. Bratzler, DO, MPH QIOSC Medical Director. Why is there a need to measure the quality of hospital care?.

E N D
Prevention of Venous ThromboembolismSurgical Care Improvement Project Dale W. Bratzler, DO, MPH President and CEO Oklahoma Foundation for Medical Quality Dale W. Bratzler, DO, MPH QIOSC Medical Director
Why is there a need to measure the quality of hospital care? • The passive strategy of guideline publication and dissemination does not effectively change clinical practice • The time lag between publication of evidence and incorporation into care at the bedside is very long • Variations in care and delivery of care that is not consistent with evidence-based recommendations is well documented Bratzler DW. Development of national performance measures on the prevention and treatment of venous thromboembolism. J Thromb Thrombolysis. 2009 (in press)
Prevention of Venous Thromboembolism (VTE) – an example • The American College of Chest Physicians published their first consensus conference on antithrombotic therapy in 1986 • In 2008 published their 8th edition of the evidence-based guideline • Despite all of these published editions….. VTE - the most common preventable cause of hospital death - 2/3 of all cases occur in recently hospitalized patients - up to 3/4 of all cases of PE death are a result of hospitalization
Prevention of Venous Thromboembolism – an example • Multiple studies that have included hospital medical record audits show consistent underuse of VTE prophylaxis • Up to 2/3 of patients with hospital-acquired VTE did not receive prophylaxis • Audits of patients receiving treatment for confirmed VTE show non-compliance with guideline-recommended treatment Bratzler DW. Development of national performance measures on the prevention and treatment of venous thromboembolism. J Thromb Thrombolysis. 2009 (in press)
“The best estimates indicate that 350,000 to 600,000 Americans each year suffer from DVT and PE, and that at least 100,000 deaths may be directly or indirectly related to these diseases. This is far too many, since many of these deaths can be avoided. Because the disease disproportionately affects older Americans, we can expect more suffering and more deaths in the future as our population ages–unless we do something about it.”
Risk Factors for DVT or PENested Case-Control Study (n=625 case-control pairs) Surgery Trauma Inpatient Malignancy with chemotherapy Malignancy without chemotherapy Central venous catheter or pacemaker Neurologic disease Superficial vein thrombosis Varicose veins/age 45 yr Varicose veins/age 60 yr Varicose veins/age 70 yr CHF, VTE incidental on autopsy CHF, antemortem VTE/causal for death Liver disease 50 0 5 15 10 20 25 Odds ratio
Surgery Trauma Immobility, paresis Malignancy Cancer therapy hormonal therapy, chemotherapy or radiotherapy Previous VTE Increasing age Pregnancy and post-partum period Estrogen-containing oral contraception or HRT or SERM Acute medical illness Heart failure Respiratory failure Inflammatory bowel disease Nephrotic syndrome Myeloproliferative disorders Obesity Smoking Varicose veins Central venous catheterization Inherited or acquired thrombophilia Travel Risk Factors for VTE Most hospitalized patients have at least one additional risk factor for VTE Geerts W et al. Chest. 2004;126:338S-400S.
VTE Facts Almost half of the outpatients with VTE had been recently hospitalized Less than half of the recently hospitalized patients had received VTE prophylaxis during their hospitalizations About half had a length of stay (LOS) of < 4 days Days After Discharge 0-29 30-59 60-90 70 60 50 40 Outpatients With VTE, % 30 20 10 0 Hospitalization with Surgery Medical Hospitalization Only Goldhaber S. Arch Intern Med. 2007;167:1451-2. Spencer FA et al. Arch Intern Med. 2007;167(14):1471-5.
Categories of Risk for Venous Thromboembolism in Patients Low risk: Minor surgery in mobile patients Moderate risk: Most medically ill, general, open gyn or urologic surgery patients High risk: Cancer surgery, hip or knee arthroplasty, hip fracture surgery, major trauma or spinal cord injury Geerts W et al. Chest. 2008;133:381S-453S.
Mechanical Methods of VTE Prevention • Graduated Compression Stockings (GCS) • Intermittent Pneumatic Compression Devices (IPCs) • Venous Foot Pump (VFP)
Pharmacologic Options for VTE Prevention • Unfractionated Heparin (UFH) • Low-Molecular Weight Heparins (LMWHs) • Pentasaccharide (Fondaparinux) • Warfarin
Prophylaxis Against Fatal Post-Operative PE With LDUH: A Multicenter, Prospective, Randomized Trial Study population: 4,121 patients age > 40 y undergoing a variety of elective major surgical procedures P < 0.005 0.9 0.77 0.8 0.7 0.6 0.5 Patients with PE (%) 0.4 0.3 0.2 0.097 0.1 0 Control (N = 2,076) UFH* (N = 2,045) • 5,000 IU SC 2 hours preoperatively and 8 hours thereafter for 7 days. Kakkar VV et al. Lancet. 1975;2:45-51.
Mechanical Thromboprophylaxis • For particularly high-risk surgery patients with multiple risk factors, pharmacologic method should be combined with mechanical method (GCS, IPC) (1C) • Use mechanical methods for patients with high bleeding risk (1A), when bleeding risk decreases substitute or add pharmacological thromboprophylaxis (1C) Geerts WH et al. Chest. 2008;133(6 Suppl):381S-453S.
Problems with Mechanical Prophylaxis • Non-compliance • ~ 50% of med-surg floors • ~80% in intensive care units • Most common reasons for non-compliance • ~80% of the time, not on the patient • ~20% of the time, on the patient but not turned on
VTE ProphylaxisGrade 1 Recommendations *Limited to those patients who have an anesthesia duration of at least 60 minutes, and a hospital stay of at least three calendar days (two nights in the hospital). *Open surgical procedure > 30 minutes requiring in-hospital stay > 24 hours postoperative.
VTE ProphylaxisGrade 1 Recommendations *Open surgical procedure > 30 minutes requiring in-hospital stay > 24 hours postoperative.
What else does the AAOS guideline say? • They do NOT recommend the use of aspirin alone • They recommend the use of mechanical prophylaxis started in the operating room or immediately postoperatively in all patients – continued to discharge • They recommend pharmacologic prophylaxis with LMWH, factor Xa inhibitor, or warfarin in high risk patients • previous history of cancer, thromboembolism, hypercoagulable states such as polycythemia, spinal cord injury patients, multi-trauma patients, and genetic predisposition
VTE Prophylaxis • Other issues • Timing of prophylaxis • Neuraxial anesthesia • Renal insufficiency • Duration of prophylaxis
Venous ThromboembolismStatement of Organization Policy “Every healthcare facility shall have a written policy appropriate for its scope, that is evidence-based and that drives continuous quality improvement related to VTE risk assessment, prophylaxis, diagnosis, and treatment.”
Electronic Submission of Performance Measures In the recently published final IPPS rule for fiscal year 2010, CMS has announced that through an interagency agreement with the Office of the National Coordinator for Healthcare Information Technology, they are developing interoperable standards for electronic medical record submission of the newly-endorsed VTE measures. Vendors of electronic medical record systems would be able to code their systems with the new specifications by the end of 2009. Centers for Medicare & Medicaid Services. Medicare Program; Changes to the Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and Fiscal Year 2010 Rates; and Changes to the Long-Term Care Hospital Prospective Payment System and Rate Years 2010 and 2009 Rates. Available at: http://www.federalregister.gov/OFRUpload/OFRData/2009-18663_PI.pdf. Accessed 10 August 2009.
Strategies to Improve VTE Prophylaxis • Hospital policy of risk assessment or routine prophylaxis for all admitted patients • Most will have risk factors for VTE and should receive prophylaxis • Preprinted protocols for surgical patients
Electronic Alerts to Prevent VTE among Hospitalized Patients • Hospital computer system identified patient VTE risk factors • RCT: no physician alert vs physician alert Control Alert group group P No. 1,251 1,255 Any prophylaxis 15 % 34 % <0.001 VTE at 90 days 8.2 % * 4.9 % 0.001 Major bleeding 1.5 % 1.5 % NS * NNT = 30 Kucher – NEJM 2005;352:969
Improving Compliance with Treatment Protocols • Use of standardized protocols, nomograms, algorithms, or preprinted orders • Address overlap (either 5 days in hospital or discharge on overlap) • When used, UFH should be managed by nomogram/protocol, and the protocol should ensure routine platelet count monitoring
Essential Elements for Improvement • Institutional support • A multidisciplinary team or steering committee • Reliable data collection and performance tracking • Specific goals or aims • A proven QI framework • Protocols SHM Resource Room. http://www.hospitalmedicine.org. Accessed September 2009.
Maynard GA, et al. J Hosp Med 2009 Sep 14. [Epub ahead of print]
Maynard GA, et al. J Hosp Med 2009 Sep 14. [Epub ahead of print]
Maynard GA, et al. J Hosp Med 2009 Sep 14. [Epub ahead of print]
Maynard GA, et al. J Hosp Med 2009 Sep 14. [Epub ahead of print]
Attention to Transitions of Care • Ensure adequate training of the patient • Education on medications, diet, follow up appointments, lab monitoring, dietary precautions, and adverse reactions or drug-drug interactions • Education for family • Referral to anticoagulation clinic • Hospital abstractors must find explicit documentation of this training/education in the chart
Changes in National PerformanceBaseline to Q1, 2009 // *National sample of 19,497 Medicare patients undergoing surgery in US hospitals during the first quarter of 2005. (Bratzler, unpublished data
Hospital-acquired ConditionsBackground of the “Never Events” • Deficit Reduction Act (DRA) of 2005 requires the Secretary of HHS to identify conditions that are: • High cost or high volume (or both); and • Result in the assignment of a case to a DRG that has a higher payment when present as a secondary diagnosis; and • Could reasonably have been prevented through the application of evidence-based guidelines.
Hospital-acquired Conditions • Deep vein thrombosis/pulmonary embolism following • Total knee replacement • Hip replacement
Conclusions • VTE remains a substantial health problem in the US • VTE prophylaxis remains underutilized • National performance measures will address both prophylaxis and treatment of VTE across broad hospital populations