KALA AZAR
KALA AZAR. DR. I. SELVARAJ I.R.M.S B.SC., M.B.B.S.,D.P.H., D.I.H.,(M.D) Community Medicine.,P.G.C H&HW(NIHFW)New Delhi Sr.D.M.O/ON STUDY LEAVE INDIAN RAILWAY MEDICAL SERVICE. SYNONYMS. kala azar, black fever, sandfly disease, Dum-Dum fever and espundia. PROMASTIGOTES. AMASTIGOTES.

KALA AZAR
E N D
Presentation Transcript
KALA AZAR DR. I. SELVARAJI.R.M.S B.SC., M.B.B.S.,D.P.H., D.I.H.,(M.D) Community Medicine.,P.G.C H&HW(NIHFW)New Delhi Sr.D.M.O/ON STUDY LEAVE INDIAN RAILWAY MEDICAL SERVICE
SYNONYMS kala azar, black fever, sandfly disease, Dum-Dum fever and espundia.
PROMASTIGOTES AMASTIGOTES
GEOGRAPHICAL DISTRIBUTION • The leishmaniasis is endemic in 88 countries on five continents—Africa, Asia, Europe, North America and South America. • 350 million people at risk. • 12 million people are affected by leishmaniasis • 1.5-2 million new cases of leishmaniasis estimated to occur annually. • 500 000 new cases of VL which occur annually
INDIA • WEST BENGAL,ANDRA PRADESH,BIHAR, ASSAM, EASTERN UTTAR PRADESH, COASTAL REGION OF TAMIL NADU, & JHARHAND • HIGHEST NUMBER OF KALA-AZAR CASES IN MADRAS CITY (18682) OCCURRED DURING THE DECADE 1951 TO 1960. THEREAFTER IT HAS SHOWN A CONTINUOUS DOWNWARD TREND. A TOTAL OF 223 CASES OF KALA-AZAR WERE REPORTED FROM 1971 TO 1983 IN MADRAS AND THE MEAN INCIDENCE OF 28 CASES WERE REPORTED BETWEEN 1971 AND 1977. FROM 1978 TO 1983 AN AVERAGE OF 4 CASES WERE REPORTED. (RECENT TRENDS IN THE INCIDENCE AND EPIDEMIOLOGY OF KALA-AZAR IN MADRAS CITY SIVAPARAKASAM, P; PADMANABHAN, B; SADANAND, AV
1756;Russel:The first description in English • 1898;Borovsky noted the protozoal nature of the organism • 1903;Leishman identified the parasite • 1903;Donovan described identical organisms in a splenic puncture
TYPES OF LEISMANIASIS • VISCERAL LEISHMANIASIS (Bangladesh, Brazil, India, Nepal and Sudan) • CUTANEOUS LEISHMANIASIS (Afghanistan, Brazil, Iran, Peru, Saudi Arabia and Syria) • DIFFUSE CUTANEOUS LEISHMANIASIS • MUCO CUTANEOUS LEISHMANIASIS (Bolivia, Brazil and Peru. • Post kala azar dermal leishmaniasis (Endemic to India and the Sudan)
Visceral leishmaniasis • irregular bouts of fever • substantial weight loss • swelling of the spleen and liver • and anaemia
CUTANEOUS LEISHMANIASIS • skin ulcers on the exposed parts of the body, such as the face, arms and legs
MUCOCUTANEOUS LEISHMANIASIS OR ESPUNDIA • mucous membranes of the nose • mouth • and throat cavities
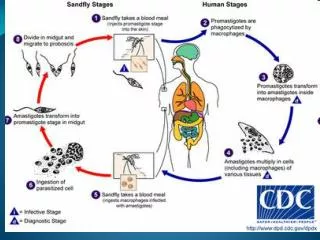
1. Leishmaniasis is transmitted by the bite of female phlebotomine sandflies. The sandflies inject the infective stage, promastigotes, during blood meals. 2. Promastigotes that reach the puncture wound are phagocytized by macrophages. 3.They transform into amastigotes. 4. Amastigotes multiply in infected cells and affect different tissues. 5. Sandflies become infected during blood meals on an infected host when they ingest macrophages infected with amastigotes. 6. In the sandfly's midgut, the parasites differentiate into promastigotes. 7. They multiply and migrate to the proboscis.
GOAL OF NATIONAL HEALTH POLICY (INDIA) 2002 ELIMINATION OF KALA AZAR 2010
STRATEGY • Interruption of transmission by reducing vector population – Indoor Residual Insecticides • Early diagnosis & treatment • Health education programme
1. To provide early diagnosis and prompt treatment; 2. To control the sandfly population through residual insecticide spraying of houses and through the use of insecticide-impregnated bed nets; 3. To provide health education and produce training materials; 4. To detect and contain epidemics in the early stages; 5. To provide early diagnosis and effective management for Leishmania/HIV coinfections.
EARLY DIAGNOSIS • L.D BODIES (SPLEEN, BONE MARROW, LYMPH NODE) • ALDEHYDE TEST • ELISA • & Polymerize chain reaction (PCR)
TREATMENT • SODIUM ANTIMONY STIBO GLUCONATE • PENTAMIDINE ISTHIONATE • AMPHOTERICIN-B • Miltefosine (Impavido ®) (approval by the Indian and German Regulatory Authorities (2003) • Phase III Trials with a first-generation vaccine (killed Leishmania organism mixed with a low concentration of BCG as an adjuvant) have also yielded promising results • Leishmania major mixed with BCG have been successful in preventing infection with Leishmania donovani.
VECTOR CONTROL • 75% DDT – 1 KG IN 3 GALLONS OF WATER OR • 50% DDT – 1.5 KG IN 3 GALLONS OF WATER • 6000 Sq. feet ( 100 mgm/Sq.foot) • Up to 6 feet from ground level • If it is resistant , BHC