Download
1 / 35
350 likes | 968 Views
NHSN Review. User Indications & Essentials. No disclosures. Objectives:. Identify mandatory reporting requirements and HAI events through case studies Utilize NHSN checklists towards final determination of HAI events

E N D
NHSN Review User Indications & Essentials
Objectives: • Identify mandatory reporting requirements and HAI events through case studies • Utilize NHSN checklists towards final determination of HAI events • Apply knowledge to determine infection classification through case studies
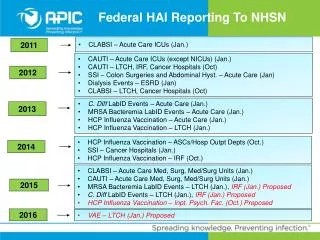
CMS Quality Reporting Programs by Care Setting Quality Programs Outside of Acute Care • 2011: CLABSI ICU • 2012: CAUTI ICU, SSI (COLO, AB/HYST) • 2013: MRSA bacteremia, C. diff. infection, HCP influenza vaccination • 2015: CLABSI & CAUTI in med, surg, and med/surg units Acute Care • 2012: CLABSI, CAUTI • 2014: HCP influenza vaccination • 2015: MRSA bacteremia, C. diff. infection • 2016: VAE Long-term acute care hospital • 2013: CLABSI, CAUTI • 2014: SSI (COLO, AB/HYST) • 2016: MRSA, C. diff., HCP influenza vaccination Cancer hospital End-stage renal disease fac. • 2012: Bloodstream infection in outpatient hemodialysis • 2015: HCP influenza vaccination Ambulatory Surgery Center • 2014: HCP influenza vaccination • 2014: HCP influenza vaccination Hospital outpatient • 2012: CAUTI • 2014: HCP influenza vaccination • 2015: MRSA bacteremia, C. diff. infection Inpatient rehab fac. Inpatient psych fac. • 2015: HCP influenza vaccination
National Data for Acute Care Hospitals, Year 2016 • CLABSI: ˅ -11% LOWER COMPARED TO NATIONAL BASELINE • CAUTI: ˅ -7% LOWER COMPARED TO NATIONAL BASELINE • MRSA Bacteremia: ˅ -6% LOWER COMPARED TO NATIONAL BASELINE • C. difficile Events: ˅ -8% LOWER COMPARED TO NATIONAL BASELINE • SSI: Abdominal Hysterectomy: ˅-13% LOWER COMPARED TO NATIONAL BASELINE • SSI: Colon Surgery: ˅ -7% LOWER COMPARED TO NATIONAL BASELINE • VAE: ˅ -2% LOWER COMPARED TO NATIONAL BASELINE
Each day, approximately one in 25 U.S. patients contracts at least one infection in association with his or her hospital care… “Healthcare-Associated Infections.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 9 Oct. 2018, www.cdc.gov/hai/data/portal/progress-report.html.
Progress by 2016 2020 Target Measure
Understanding & Application of NHSN Surveillance Definitions • IP group within healthcare system • March – October 2017 • Case Studies - CAUTI & CLABSI • Identification elements: Definition met, IWP, DOE, RIT, SBAP • April 2017 (baseline) October 2017 (comparison) Same scenario but different dates & organisms • Challenged by intricacies of NHSN definitions, but with persistent review competency increases Adams, Jennifer, and Teri Mauldin. “How Well Do Infection Preventionists Understand and Apply the National Healthcare Safety Network Surveillance Definitions?” American Journal of Infection Control, vol. 46, no. 6, June 2018, doi:10.1016/j.ajic.2018.04.095.
Accuracy & Consistency • Assess application of standardized surveillance definitions: • 2010 – 2016 • 22 cases studies – 7,950 respondents • Consistency: • Correct responses – 62.5%, but with wide range • Respondents self-identified – IP, Physician or Public Health Professional • Accurate application of surveillance criteria was suboptimal, highlighting need for continuing education, competency development, and auditing Wright, Marc-Oliver, et al. “Assessment of the Accuracy and Consistency in the Application of Standardized Surveillance Definitions: A Summary of the American Journal of Infection Control and National Healthcare Safety Network Case Studies, 2010-2016.” American Journal of Infection Control, vol. 45, no. 6, 2017, pp. 607–611., doi:10.1016/j.ajic.2017.03.035.
Case Study On April 7th, a 50 year old female was admitted to the Intensive Care Unit following a CVA. A Foley catheter and central line were placed. April 8th, the patient’s temperature was 100.9°F and a urine culture grew 10,000 cfu/ml of Pseudomonas aeruginosa. April 9th – 10th, the patient was stable with her family at her bedside.
April 11th, the Foley and central line were removed and the patient was transferred to the medical surgical unit. April 12th, the patient complained of dysuria. April 15th, she had a temperature of 100.2°F, urine culture grew > 100,000 cfu/ml Pseudomonas aeruginosa and >100,000 cfu/ml Candida albicans.
Question 1 Does this patient have a CAUTI? If so, what is the Date of Event? • Yes, SUTI 1a with DOE of 4/15 • No • Yes, SUTI 1a with DOE of 4/12 • Yes, ABUTI with DOE of 4/15
Question 2 What organism(s) is/are reported for the CAUTI? • Pseudomonas aeruginosa • Candida albicans • Pseudomonas aeruginosa and Candida albicans
DOE – 4/12 IWP – 4/12-4/18 RIT – 4/12-4/25 SBAP – 4/12-4/25
Case Study On March 9th, an 18 year-old male is admitted to a pediatric medical ward. He has coarse breath sounds over the right upper lobe of the lung, O2 saturations are at 86% and he is started on oxygen therapy at 4 liters/min. Chest x-rays collected on admission show diffuse bilateral bronchiectasis, worse in the right upper lobe, with parenchymal opacities which may represent atelectasis, but most likely represent superimposed pneumonia. The left lung is clear. His white blood cell count is elevated at 16,000.
On March 10th, the patient develops a fever of 101.4°F, and pulmonary crackles are heard over the upper right lung. Sputum, which is now blood-tinged, is collected for culture. The patient is tachypneic and is placed on a conventional mode of mechanical ventilation. On March 11th, fever, crackles and tachypnea continue, and the patient is coughing up large amounts of green sputum. FiO2 settings range between 30-100%. A triple lumen catheter is placed in the subclavian vein.
On March 12th, the sputum culture collected on March 10th is reported positive for Staphylococcus aureus and Pseudomonas aeruginosa. On March 13th, another chest x-ray is obtained, which shows an increased, confluent opacity in the right upper lobe, and the radiologist states that pneumonia is likely. Patient remains on mechanical ventilation.
Question 1 - Patient meets: • PNU1 criterion, clinically defined pneumonia, DOE March 9thand the event is not ventilator associated • PNU1 criterion, clinically defined pneumonia, DOE March 9th and the event is ventilator associated • PNU2 criterion, pneumonia with common bacterial or filamentous pathogens and specific laboratory findings, DOE March 10th • PNU2 criterion, DOE March 12th
DOE – 3/9 IWP – 3/7-3/12 RIT – 3/9-3/22 SBAP – 3/7-3/22
Scenario Continued… On March 15th, the patient’s WBC remains elevated, at 14,800. On March 16th, rales are again documented, the his temperature increases to 103.1°F and blood is collected for culture. The patient continues to have thick creamy green sputum. A follow up chest x-ray shows continued dense opacities in the upper lobe of the right lung. On March 17th, the blood culture is reported positive for S. aureus.
Question 2 Does this patient have a CLABSI with S. aureus?? • Yes, this patient has a CLABSI - DOE March 16th • Yes, this patient has a CLABSI - DOE March 17th • No, the bloodstream infection is secondary to PNU1. • No, the bloodstream infection is secondary to PNU2.
PNU2 Infection Window Period (based on diagnostic test – 3/13) DOE –3/9; 3/13 IWP – 3/7-3/12 RIT – 3/9-3/22 SBAP – 3/7-3/22
Upcoming Changes…. • CLABSI exclusions • NHSN Outpatient Procedure Component • Introduction of Pediatric Ventilator-Associated Event (PedVAE) • New Name for Clostridium difficile
ECMO/VAD Central Line-Associated BSI Exclusion, 2019 Reporting of these events are required This exclusion is met if: • Eligible central line in place • Central line accessed on an inpatient unit > 2 consecutive calendar days • VAD and/or ECMO support in place greater than 2 days on the bloodstream infection (BSI) date of event, or the day before
*Optional* CLABSI Exclusion Criteria • Epidermolysis bullosa (EB) • Munchausen Syndrome by Proxy (MSBP) • IV Drug Abuse (IVDA) • Pus at the Vascular Access Site • Group B Streptococcus (GBS) • Watch for CLABSI Exclusion Table: 2019
NHSN Outpatient Procedure Component (OPC) • Scheduled for launch Nov 1 • Specifically for ASCs • Hospital Outpatient Departments (HOPDs) are not included • OPC replaces use of Patient Safety Component for ASC SSI reporting • Two modules: 1) Same Day Outcome Measures 2) Surgical Site Infection • Training Materials & Protocols Available Soon
Pediatric Ventilator-Associated Event (PedVAE) • Cocoros NM, Kleinman K, Priebe GP, et al. Ventilator-Associated Events in Neonates and Children--A New Paradigm. Crit Care Med. 2016 Jan;44:14-22. • On target for reporting events • Difference from Adult VAE > single tier! • Use of FiO2 ventilator settings and Mean Airway Pressure (MAP) values as criterion • PedVAE Calculator planned release 2019
New Name for Clostridium difficile • Clostridium difficile to Clostridioides difficile • Abbreviations will NOT change • NHSN implementation of change • Documents dated prior to January 1, 2019 – retain former name • Documents dated after January 1, 2019 – incorporate new name • NHSN application Δ on or after April 2019
Lela L Luper, RN, BS, CIC, FAPIC Infection Preventionist Institutional Environmental Health the Chickasaw Nation 1921 Stonecipher Blvd. Ada OK 74820 Office (580)421-2984 lela.luper@Chickasaw.net
Citations: Adams, Jennifer, and Teri Mauldin. “How Well Do Infection Preventionists Understand and Apply the National Healthcare Safety Network Surveillance Definitions?” American Journal of Infection Control, vol. 46, no. 6, June 2018, doi:10.1016/j.ajic.2018.04.095. Allen-Bridson, Katherine, et al. “Health Care-Associated Infections Studies Project: An American Journal of Infection Control and National Healthcare Safety Network Data Quality Collaboration.” American Journal of Infection Control, vol. 45, no. 12, 2017, pp. 1394–1395., doi:10.1016/j.ajic.2017.09.011. “HAI Checklists | NHSN | CDC.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 2018, www.cdc.gov/nhsn/hai-checklists/index.html. “Healthcare-Associated Infections.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 9 Oct. 2018, www.cdc.gov/hai/data/portal/progress-report.html. “National Healthcare Safety Network (NHSN) Patient Safety Component Manual.” Centers for Disease Control and Prevention, 2018, www.cdc.gov/nhsn/pdfs/pscmanual/pcsmanual_current.pdf. “National Targets and Metrics.” National Targets and Metrics - Health Care-Associated Infections, 9 Oct. 2018, health.gov/hcq/prevent-hai-measures.asp. “Newsletters | NHSN | CDC.” Centers for Disease Control and Prevention,2018, www.cdc.gov/nhsn/newsletters/index.html. Powell, LaTasha, et al. APIC NHSN Webinar October 18, 2018. Live Webinar of NHSN Update Fall 2018, 2018, webinars.apic.org/webcast/login.php?ft=s&id=27017. Wright, Marc-Oliver, et al. “Assessment of the Accuracy and Consistency in the Application of Standardized Surveillance Definitions: A Summary of the American Journal of Infection Control and National Healthcare Safety Network Case Studies, 2010-2016.” American Journal of Infection Control, vol. 45, no. 6, 2017, pp. 607–611., doi:10.1016/j.ajic.2017.03.035. Wright, Marc-Oliver, et al. “Healthcare-Associated Infections Studies Project: An American Journal of Infection Control and National Healthcare Safety Network Data Quality Collaboration.” American Journal of Infection Control, vol. 38, no. 5, June 2010, pp. 416–418., doi:10.1016/j.ajic.2010.04.198.