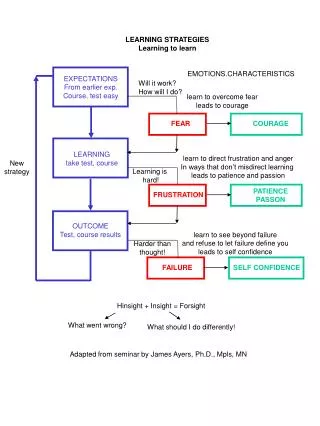
Learning to learn from accidents..
Presented by:. Roger Bibbings MBE, BA, CFIOSH, Occupational Safety Adviser THE ROYAL SOCIETY FOR THE PREVENTION OF ACCIDENTS. Learning to learn from accidents. RoSPA’s Mission & Vision. Mission To save lives and reduce injuries Vision To lead the way in accident prevention.

Learning to learn from accidents..
E N D
Presentation Transcript
Presented by: Roger Bibbings MBE, BA, CFIOSH, Occupational Safety Adviser THE ROYAL SOCIETY FOR THE PREVENTION OF ACCIDENTS Learning to learn from accidents..
RoSPA’s Mission & Vision Mission To save lives and reduce injuries Vision To lead the way in accident prevention
Health and safety failure: UK PLC • 241 notified fatal injuries to workers (06/07) • 100 + members of the public • 1,000 fatal WoRRIs? • 328,000 reportable injuries (LFS 06/07) • 24,000 deaths (?) due to work related health damage • 1 million injuries (all severities) • 2 million cases of work related ill health • 36 million working days lost • £20 – 30 billion or between 2 –3 % of GDP!
Or… • One crashing every fortnight (fatals/early death) • Twenty landing every day (injuries/ill-health)
RoSPA’s key issues in OS&H • Director leadership • Learning from accidents • Managing occupational road risk • SMEs • 24/7 safety
Aims of presentation • Brief you on RoSPA’s ‘key issue’ work on ‘learning from prevention failure’ • Provide RoSPA’s views on HSE’s approach • Review opportunities and barriers • Examine the case for team based investigation • Brief you on Project DORI • Invite YOUR views on the way ahead!
Windscale (Sellafield) – RadiationBritish Nuclear Fuels30 estimated fatalities Abervan, – Coal Tip National Coal Board144 fatalities Kings Cross Station - FireLondon Underground31 fatalities Flixborough, ExplosionNypro 18 fatalities Piper Alpha - Fire/ExplosionOccidental Phillips167 fatalities Herald of Free Enterprise - Townsend Thoresen193 fatalities 1966 1987 1987 1957 1974 1988 Three decades of disasters
2000 Kegworth, UK – Plane CrashBritish Midland47 fatalities Southall Train Crash –Railway Operator7 fatalities Lyme Bay - Canoeing AccidentOLL Ltd4 fatalities Paddington Rail CrashRailway Operator28 fatalities Glasgow, Scotland – ExplosionICL Plastics9 fatalities Grangemouth, Scotland – ExplosionBritish Petroleum2 fatalities 1993 1997 2004 1988 2004 And another two decades
BP Texas City Refinery Accident 2005: 15 dead, 170 injured $21 million fine destroyed shareholder value CEO + senior managers left high regulatory scrutiny Board did not validate effective health and safety management or strive for excellence lack of a common unifying health and safety culture over-reliance on measures of personal v process safety failure to analyse lead/lag indices of process safety James Baker Lessons from Baker Report
Why accident investigation is so fundamental • OS&H management theory now focused on proactivity and risk assessment • In reality much new action is still reactive • BUT many organisations fail to extract full value from investigation • They fail to turn reactivity into proactivity • Accident investigation remains an underdeveloped part of OS&H management.
The essence of investigation • Reporting, emergency action, securing scene • Initial appraisal, scaling response, agreeing ToR etc • Evidence gathering (interviews, photos, material evidence etc) • Integrating evidence (structured methods, ECFA, MORT etc) • Generating and testing hypotheses (what, who, when, how, why etc?) • (Searching for further evidence) • Reaching conclusions • Making recommendations • Tracking closure • Reviewing process
Common pitfalls • No investigation at all (+ RIDDOR under-reporting) • No reporting/investigation of ‘near -misses’ • No procedures • Lack of clarity about purposes • No scaling/prioritisation of effort • Little/no managerial or worker involvement • Concluding the investigation too early • Automatically blaming the victim • No examination of underlying organisational factors • No/poor communication of lessons learned
Uni-causal view of events Focus on fault and blame Two big underlying problems
A B C D F G H I J E Think about causation
Think about error • Taxonomy of human error • ‘Slips’ and ‘lapses’ • ‘Mistakes’ – skill and/or rule based • ‘Violations’ – exceptional, routine and situational
Reason’s swiss cheese model Accident trajectory Organisational Barrier Technological Barrier Behavioural Barrier Accident trajectory
HSE Contract Research Report 344 Accident investigation – the drivers, methods and outcomes (2001):www.hse.gov.uk/research/crr_pdf/2001/crr01344.pdfMain findings • Companies employ a range of approaches from unstructured, ad hoc approaches to well supported ones with procedures, tools and techniques. • Approaches used causal models from system-based to traditional models • Despite limitations, vast majority of companies still consider that they have a structured approach • Limited resources allocated - little/no senior managerial, worker or worker rep. involvement • Likelihood of sophisticated approaches increased with size of company
HSE Contract Research Report 344: Barriers • Current and developing legal environment • Potential isolation of accident investigation from risk assessment • Lack of common model & structure to support incident investigation • Current low level of competence, lack of training and complacency in companies • Resource implications of improving standards, particularly for small companies
RoSPA’s perspective • AI is an under-developed part of H&S management • ‘Self regulation’ not possible without organisational safety learning • AI can improve understanding of OH&S management • Accidents are organisational learning opportunities • Poor AI policy and practice a reflection of failure to popularise contemporary views of OH&S management • Accidents are emotionally charged and the adversarial basis of litigation is a barrier to effective AI • Valuable texts and materials are available but do not meet current needs
Our aims • Initiate new national debate • Generate consensus • Stimulate new initiatives • Promote more robust approaches • Strengthen role of investigation in SMS • PROMOTE MORE EFFECTIVE ORGANISATIONAL SAFETY LEARNING FROM ACCIDENTS/INCIDENTS
RoSPA initiatives • Advice from reference group • RoSPA discussion document (1998) • Congress presentations • ‘One-to-one’ discussions (TUC, CBI etc) • Partner in HSC discussion exercise (1998) • ‘High performers’ review (1999) • Response to HSC consultation • RoSPA ‘Challenge’ (2002) • Input to new Annexe G in BS 8800 (2002) • Input to HSE Guidance (2003) • DORI/PRIA (2005/6)
‘One-to-one’ discussions with ‘key players’ • IOSH, FSB, EEF, TUC, CBI, APIL, ABI, HSE (OU), LPC • General agreement about: • poor state of current practice • learning potential of good investigation • need for better guidance/training/support • A variety of views about: • litigation etc as a barrier • the need for legislation
HSC proposals for a more explicit duty to investigate… • Amendment to MHSW Regs • RIDDOR notifiable events to be investigated by ‘responsible person’ • Covered accidents, dangerous occurrences, notifiable diseases • Investigation to be started no later than 3 days after date at which event to be notified • Safety reps to participate • Review risk assessments and keep records • Inform others of implications • Inform safety reps
RoSPA’s views.. • Duty to investigate already implicit in HSW Act and MHSW Regs • Amendment to MHSW Regs could help to make this explicit • Investigation is ‘Management system’ not ‘RA’ territory! • Goal setting duties backed by ACoP (not RIDDOR linked!) • Clearer guidance needed
Seven reasons why investigation duty should NOT be RIDDOR linked • RIDDOR’s purpose is to provide intelligence to HSE • Perpetuates myth that scale/scope of investigation is outcome linked • SME RIDDOR problems, under-reporting • DO schedule very limited • Interval between RIDDOR events too long • Three days absence introduces delay • Prescription does not challenge employers to develop own criteria
HSE guidance (HSG245) 'Investigating accidents and incidents - a workbook for employers, unions, safety representatives and safety professionals' (HSG245) July 2004 (‘the gathering of information; the analysing of information; identifying risk control measures;and the action plan and its implementation’)
RoSPA’s ‘High Performers’ Review • Powergen, CCG (UK), Haden Young, Kellogg’s, Foster Wheeler, Shell Expro, Scottish Hydro • Aims: • provide illustration of ideas in the RoSPA discussion document • demonstrate the ‘art of the possible’ • probe perceptions of AI within companies • inform the wider debate
Main findings • Effective investigation rests on strong reporting culture • Informal problem solving sets pattern for more structured investigation • Tackling the aftermath of accidents requires maturity and robust relationships • Team based investigation offers significant advantages
Why ‘team based’ adds value • Sharing knowledge and perspectives • Team building and trust • Supporting ‘just’ cultures • Learning how to investigate • Linkage to closure • Investigation as a complement to audit • Developing understanding of risk management in practice • Developing risk literacy • Creating more champions for OS&H change
First aid/rescue Making safe Preserving/managing the scene RIDDOR Informing/liaising Dealing with authorities Investigation, learning and remediation Coping with the aftermath Accidents test your organisation
HSE, Lawyers Other public authorities Families, Insurers, Workforce, Trades unions Customers/clients, The media Informing /liaising
Investigations by Police HSE, LAs etc Interviews under caution Seizure of evidence Enforcement action Notices Prosecutions Enforcer intervention
HSW ACT Sections 2, 3 etc Section 7 Section 37 (‘consent, connivance or neglect’) MHSW regs (risk assessment etc) Specific regs (COSHH, MH, LOLER) Corporate Manslaughter Manslaughter Prosecution options
Damage costs Sick pay Replacement staff/equipment Business interruption, delays, lost contracts etc Loss of workforce morale Reputational loss Fines Compensation payments Higher insurance premia Career damage? Assessing impact
See accidents as an investment Exploit unique learning/change opportunities See accidents as ‘windows on reality’ Build trust through team based investigation Learn from near misses/hits But accidents/incidents are also opportunities
4 2 1 3 Same unplanned event, different outcomes • Near miss • Damage • Minor injury • Fatality
Fatal Very serious Serious Slight Damage only Near misses Failure of controls Unsafe acts / conditions Outcome ratios
Operational readiness is key • Create an organisation that • places the right people • in the right places • at the right times • working with the right hardware • according to the right procedures and management controls • At a secondary level, readiness implies that the needed elements are functioning in a conducive physical and psychological environment
If not ready • Threat to the relationships between stakeholders • Response not geared to requirement to learn • Lack of clarity about what happened • Poor handling of evidence, including witnesses • Uneven analysis and interpretation • Tendency to allocate blame • Poor rates of near-miss/near hit reporting • Lack of continual improvement • Poor quality of remedial change and learning
Project DORI (Definition of Operational Readiness to Investigate) • Defining Operational Readiness to Investigate • Partnership between RoSPA and NRI Foundation • Proposed Outputs: • functional analysis of investigation • criteria for readiness to investigate • list of phases for developing readiness • basis for subsequent RoSPA project, “PRIA” (Programme for Readiness to Investigate Accidents) • Final report published as a ‘White Paper’ on the NRI Foundation website (www.nri.eu.com)
Collecting (early) statements Assigning investigation level Selecting the team Developing terms of reference Enabling/protecting the team Managing the team Liaising with other teams Cataloguing evidence Recording visual data Collecting document, logs, equipment, material and environmental evidence Interviewing witnesses What happened and how Alternative lines of enquiry Evaluate/testing hypotheses Identifying controls and barriers Identifying root causes Writing reports Developing remedial actions Reviewing the investigation Debriefing the team Debriefing affected staff/others Managing recommendations Returning, archiving or disposing of evidence Practical readiness issues
Some parting thoughts… • Accidents as emotionally charged experiences? • ‘Tell it all, tell it early’? • Developing a proportional approach? • Understanding causal factors - not cause • Investigation as a general management skill • Developing ‘an investigation culture’ • Seek team based ‘tap in/buy in’?
Top tips for teams • Director/senior manager led • Early review/confirmation of of ToR • Safety reps and other contributors • Training in investigation techniques • Evidence gathering/integration • Witness interview techniques • Safety advisers as ‘process doctors’ • Separation from common law claims
Some ideas for organisations • Review existing procedures against the RoSPA ten points or BS 8800 Annexe G? • Coverage in 2009 programmes? • ‘Accident of the month’? • Review training/awareness raising? • Establishing ‘lessons learned’ databases? • ‘Mentoring’/hand holding (contractors)? • ‘Swapping’ investigation teams? • Developing support services via trade associations etc? • Participate in DORI?
And finally Good investigation shows most accidents are preventable and counters the assertion that..
‘Elf and safety has gorn mad?’ • ‘‘Every week we have more evidence of the slimy, choking advance of jobsworth regulation which seeks to make us “safe” but actually makes us weak.’ (Libby Purves, broadcaster) • ‘Our national attitude to risk is becoming defensive and disproportionate;…Britain must safeguard its sense of adventure, enterprise and competitive edge.” (Better Regulation Commission)
But please.. don’t have nightmares