Download
1 / 27
320 likes | 830 Views
Anticoagulants and Thrombolytic. Objectives. To learn how Blood Clots are formed. How the blood clots are broken down ? What drugs can be used to regulate clotting ? How to rectify clotting deficiencies. Classes of Drugs. Prevent coagulation Dissolve clots

E N D
Objectives • To learn how Blood Clots are formed. • How the blood clots are broken down ? • What drugs can be used to regulate clotting ? • How to rectify clotting deficiencies
Classes of Drugs • Prevent coagulation • Dissolve clots • Prevent bleeding and hemorrhage - Hemostatic • Overcome clotting deficiencies (replacement therapies)
Blood Clotting • Vascular Phase • Platelet Phase • Coagulation Phase • Fibrinolytic Phase
Vascular Phase • Vasoconstriction • Exposure to tissues activateTissue factor and initiate coagulation Tissue Factor
Platelet phase • blood vessel wall (endothelial cells) prevent platelet adhesion and aggregation • platelets contain receptors for fibrinogen and von Willebrand factor • after vessel injury Platelets adhere and aggregate. • Release permeability increasing factors (e.g. vascular permeability factor, VPF) • Loose their membrane and form a viscous plug
Coagulation Phase • Two major pathways • Intrinsic pathway • Extrinsic pathway • Both converge at a common point • 13 soluble factors are involved in clotting • Biosynthesis of these factors are dependent on Vitamin K1 and K2 • Normally inactive and sequentially activated • Hereditary lack of clotting factors lead to hemophilia -A
Intrinsic Pathway • All clotting factors are within the blood vessels • Clotting slower • Activated partial thromboplastin test (aPTT) Extrinsic Pathway • Initiating factor is outside the blood vessels - tissue factor • Clotting - faster - in Seconds • Prothrombin test (PT)
Intrinsic Pathway Extrinsic Pathway Tissue Injury Blood Vessel Injury Tissue Factor XIIa XII Thromboplastin XIa XI IXa IX VIIa VII Xa X X Prothrombin Thrombin Factors affected By Heparin Fribrin monomer Fibrinogen Fibrin polymer Vit. K dependent Factors Affected by Oral Anticoagulants XIII
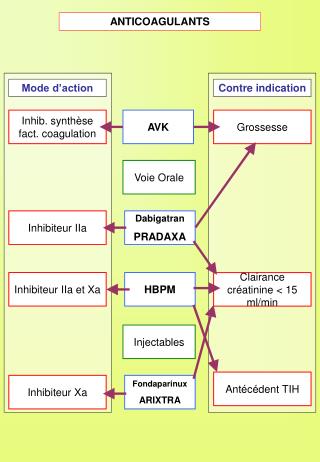
Anticoagulant drugs to treat thromboembolism Drug Class Prototype Action Effect Anticoagulant Parenteral Inactivation of clotting Factors Heparin Prevent venous Thrombosis Anticoagulant Oral Warfarin Decrease synthesis of Clotting factors Prevent venous Thrombosis Prevent arterial Thrombosis Antiplatelet drugs Aspirin Decrease platelet aggregation Breakdown of thrombi Thrombolytic Drugs Streptokinase Fibinolysis
Heparin • Sulphated carbohydrate • Different sizebovine lungs • Administration - parenteral- Do not inject IM - only IV or deep s.c. • Half-life 1 - 5 hrs - monitor aPTT • Adverse effect: hemorrhage • Antidote : protamine sulphate
Heparin mechanism of action Heparin Antithrombin III Thrombin
Oral anticoagulants • Examples: Coumarins - warfarin, dicumarol • Structurally related to vitamin K • Inhibits production of active clotting factors • Clearance is slow - 36 hrs • Delayed onset 8 - 12 hrs • Overdose - reversed by vitamin K infusion • Can cross placenta - do not use during late pregnancies
Mechanism of action Descarboxy Prothrombin Prothrombin Reduced Vitamin K Oxidized Vitamin K NAD NADH Warfarin Normally, vitamin K is converted to vitamin K epoxide in the liver. →This epoxide is then reduced by the enzyme epoxide reductase. →The reduced form of vitamin K epoxide is necessary for the synthesis of many coagulation factors (II, VII, IX and X, as well as protein C and protein S). →Warfarin inhibits the enzyme epoxide reductase in the liver, thereby inhibiting coagulation. (عبدالله المطيري)
Warfarin Side Effect • Severe Side effects: • Severe bleeding • Bleeding from the rectum or black stool • Skin conditions such as hives, a rash or itching • Swelling of the face, throat, mouth, legs, feet or hands • Bruising that comes about without an injury you remember • Chest pain or pressure • Nausea or vomiting • Fever or flu-like symptoms • Joint or muscle aches • Diarrhea • Difficulty moving • Numbness of tingling in any part of your body • Painful erection lasting four hours or longer
Warfarin Side Effect • Other less serious warfarin side effects: • Gas • Feeling cold • Fatigue • Pale skin • Changes in the way foods taste • Hair loss
Drug interaction- with Warfarin Category Mechanism Representative Drugs Drugs that Increase Warfarin Activity Decrease binding to Albumin Inhibit Degradation Decrease synthesis of Clotting Factors Aspirin, Sulfonamides Cimetidine, Disulfiram Antibiotics (oral)
Drug interaction with Warfarin Drugs that promote bleeding Inhibition of platelets Aspirin Inhibition of clotting heparin Factors antimetabolites Induction of metabolizing Barbiturates Enzymes Phenytoin Promote clotting factor Vitamin K Synthesis Reduced absorption cholestyramine colestipol Drugs that decrease Warfarin activity
Antiplatelet drugs • Example: Aspirin • Prevents platelet aggregation /adhesion • Clinical use - prevents arterial thrombus • Myocardial infarction (MI), stroke, heart valve replacement and shunts • Other antiplatelet drugs are - Dipyridamole, sulfinpyrazone and Ticlopidine
Mechanism of action • Aspirin inhibits cyclooxygenase (COX) • COX is a key enzyme involved in the synthesis of thromboxane 2 (prostaglandins) • Inhibits platelet aggregation
Prophylactic use of Aspirin • Low dose daily. • Prevents ischemic attack (ministroke) and MI • 335 mg/day reduced the risk of heart attack in patients over 50 • More than 1000 mg/day NO EFFECT • Contraindication - DO NOT give to patients with glucose 6-PO4 dehydrogenasedeficiency
Fibrinolysis • Enhance degradation of clots • Activation of endogenous protease • Plasminogen (inactive form) is converted to Plasmin (active form) • Plasmin breaks down fibrin clots
Fibrinolysis • Exogenously administered drugs • Streptokinase - bacterial product • - continuous use - immune reaction • Urokinase - human tissue derived – • no immune response • Tissue plasminogen activator (tPA) - genetically cloned • no immune reaction • EXPENSIVE
Drug preparations : To reduce clotting • Heparin (generic, Liquaemin sodium) • Parenteral - 1000 - 40,000 U/ml • Warfarin (generic , Coumadin) • Oral : 2 - 20 mg tablets • Dipyridamole (Persantine) • Oral : 25,50,75 mg tablets
Drug preparations : to lyse clots • Alteplase recombinant (tPA, Activase) • 20, 50 mg Lyophilized powder - reconstitute for iv • streptokinase (Kabikinase, streptase) • Parenteral : 250000 - 1.5 million units per vial . Lyophilized powder. Reconstitute for iv • Urokinase ( Abbokinase) • Parenteral : 250000 units per vial. Powder to reconstitute to 5000 u/ml for injection
Drug preparations: clotting deficiencies • Vitamin K ( Phytonadione (K1), Mephyton • Oral : 5 mg tablets • Plasma fractions - for hemophilia • Antihemophilic factor ( VIII, AHF) • Parenteral • Factor IX complex (konyne HT, proplex T) • Parenteral : in vials
Drug preparations : to stop bleeding • Systemic use : aminocaproic acid (Amicar); Tranexamic acid (cyclokapron),Vitamin K • Local adsorbable drugs • Gelatin sponge (Gelfoam) • Gelatin film • Oxidized cellulose ( Oxycel) • Microfibrillar collagen (Avitene) • Thrombin