Download
1 / 18
250 likes | 2.83k Views
The Ophthalmic disorder : Uveitis Presented by Abdulaziz . M. Al - Saad Introduction Definition : Inflammation of the uveal tract ( the iris, ciliary body and choroid ). Anatomical Classification : 1. Inflammation of the iris ( iritis or anterior uveitis ).

E N D
The Ophthalmic disorder : Uveitis Presented by Abdulaziz . M. Al - Saad
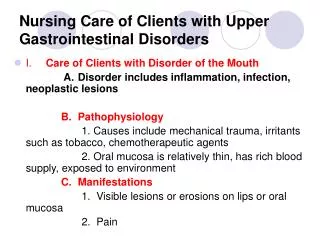
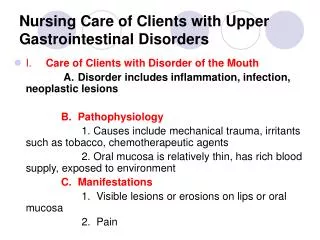
Introduction Definition :Inflammation of the uveal tract ( the iris, ciliary body and choroid ). Anatomical Classification : 1. Inflammation of the iris ( iritis or anterior uveitis ). Accompained by increase vascular permeability: • White cells ciculasting in aqueous humour of anterior chamber • Proteins Picked out by its light scattering properities( in the beam of slight light ) . 2. Inflammation of the pars plana ,posterior ciliary body, ( Cyclitis or Intermediate uveitis ). 3. Inflammation of the posterior segment ( Posterior uveitis ) . • Inflamtory cells in the vitreous gel. 4. Inflammation of choroid or retina ( choroiditis and retinitis ). 5- Inflammation of anterior and posterior uveitis together ( Panuveitis ).
Epidemiology • Incidence of uveitis : 15 per 100 000 people. 75 % of these are Interior uveitis. - About 50 % of patients, have an associated systemic disease.
History The patient complain , include : 1- Ocular pain ( less with posterior uveitis or choroiditis ) 2- Photophobia . 3- Blurred vision . 4- Redness of the eye . Note :The patient must be questioned about relevant symptoms , that may help in the determination of whether or not there is associated systemic disease : 1- Respiratory System : Shortness of breath, Cough, Nature of sputum ( associated sacoidosis or tuberclusis). 2- Bowel Disease : Occasionallyt uveitis may be associated with ulcerative colitis, cron,s disease and whipples disease.
3-Skin Problems : 1. Erythema nodosum ( Painfull raised red lesions on the arm and legs ), present in agranulomatous disease such as sarcodosis and Behcet,s disease . 2. Patint with Behcets disease may also have : thrombophlebitis, dermtographia, oral and genital ulceration . 3. Psoriasis ( in association with arthritis ) may be accompained by uveitis . 4- Joint disease : AAU : associated with Ankylosing spondylitis with back pain . In children : juvenile chronic arthritis may be associated with uveitis Reiter,s disease ( classically urethritis, conjunctivitis and seronegative arthritis ) may be associated with anterior uveitis . 5- Infectious Disease : Syphilis with its protean manifestation can cause uveitis ( es. Posterior choroiditis ) Herpetic disease ( shingles ) may cause uveitis. Cytomegalovirrus (CMV ) may cause uveits ( es. In patient with AIDS Fungulinfections and metastatic infections may cause uveitis ( usyally in immunocompromised patient )
Signs On examination : 1- Decrease visual acuity . 2- Eye will be inflammed in acute anterior disease . 3- Inflamatory cells may be visible clumped together on endothelium of cornea ( es. Inferiorly )( Keratitic pps ). 4- Slight lamp examination : reveal aqueouscells and flare. If inflammation sever , White cells collect as a mass inferiorly ( hypopyon ) 5- Dilatation of vessels on the iris . 6- Iris may adhere to lens ( posterior synechiae or PS ). 7- IOP may be elevated. 8- cells may be present in the vitreous. 9- retinal or choroidal foci of inflammation may be present . 10- Macular odema may be present .
Investigation Aimed at determining a systemic association and are directed in part by the type of uveitis. A. Anterior Uveitis : • More likely associated with ankylosing spondylitis and HLA-typing may help to confirm diagnosis . • Presence of large KPs and nodules on iris suggest sarcoidosis; a chest radiograph, serum calcium and serum angiotensin converting enzym would be appropriate • In toxoplasmic retinochoroiditis , the focus of inflammation ofen at margin of an old inflammatory choroidal scar. B. Posterior Uveitis : - May have an infectious or systemic inflammatory cause - Disease such as CMV in HIV- positive patients have characteristc appearance with appropriate history ( no need for further diagnostic test ) - Associated symptomns may help toward systemic disease ( e.g. fever, diarrhoea, weight loss ) NOTE : Not all case of anterior uveitis requir investigations at first presentation unless systemic symptoms are present .
Treatment • Goals of treatment : • 1- Relieveing pain and inflamation in the eye. • 2- Preventing damage to ocular structures. • 3- Preventing visual loss due to retinal or optic nerve damage. • Pharmacological treatment • Anterior Uveitis : • Dilatation of the pupil prevent the formation of Posterioor Synechiae , by separating it from the anterior lens capsule. ( Synechiae interfer with normal dilatation of pupil ) . • Dilatation is achieved by :Homatropine, Cyclophentolate or Atropine drops. ( Atropine > prolonged action ) • To break any synechiae , start with intensive initial Cycophentolate, Phenylepherine , and Tropicamide drops. • - Subconjunctival injection of mydriatics may help to break resistant synechiae.
B. Posterior Uveitis : • Visual loss may occur due to destructive processes caused by : • 1- Retina it self ( e.g. in toxoplasma or CMV ) OR • 2- Fluid accumulation in the layers of the macula ( Macular Odema ) • This require antiviral or antibiotic or systemic steriod therapy • Some rare but sever form of uveitis e.g. that associated with Behcet,s disease requir systematic immunosuppressive drugs such as : Azathioprine , or Cyclosporine . • Longe term therapy may be necessary
Specific Conditions Associated with Uveitis There are a large number of systemic disease associated with Uveitis :
SpecialConditions Ankylosing spondylitis Definition: Seronegative ( RF – ve ) inflamatory arthritis of the spine . Signs : Typical of anterior uveitis. Treatment : Ocular treatment + intermittent anti-inflammatory + Physiotherapy. Prognosis : Recurrent attack . The out look for vision is good ( if acute attack treated early & vigorously ). Juvenile chronic arthrits Definition : A seronegative arthritis which present in children , either systemic disease with fever and lymphadenopathy, particular or polyparticular arthritis. Signs : white eye + signs of an anterior uveitis + cataract + glucoma ( due to uveitis or steroid drops . Treatment : Ocular treatment + systemic treatment for joint disease + glucoma difficult to be treated ( if medication fail , syrgery may be required ).
SpecialConditions Toxoplasmosis The infection may be congenital or aquired ( 50-75 % congenital ) Treatment : - Reactivated lesions will subsidebut treatment is required if macula or optic nerve is threatened or if the inflammatory response is very severe. + systemic steroids are adminstered with antiproto zoal e.g. clidamycin ( care for pseudomembranous colitis from clindamycin ) ( patient should be warned that if diarrhoea dvelops they should seek medical help immediately )
Patient Informations 1,2 : • Take all medication , don’t skip doses , • Take it 1 hr befor or 2 hr after meals [ Enhance F ] . • Missed dose- take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses. • Storage : • Keep out of the reach of children. • Store away from heat and direct light. • Do not store the capsule or tablet form of penicillins in the bathroom. Heat or moisture may cause the medicine to break down. • Store the oral liquid form of penicillins in the refrigerator because heat will cause this medicine to break down. However, keep the medicine from freezing. Follow the directions on the label. • Do not keep outdated medicine or medicine no longer needed. Be sure that any discarded medicine is out of the reach of children.
Stability 3 : 1. Methicillin : - Sensetive to moisture --- Loss ½ of its activity after 5 days at RT . - Solution for parental ad. May kept for 24 hr ----- [ at 5oC ] . 2. Nafcillin , Oxacillin : Parentral sol. Stable for 3 days at RT. ( 96 hr if ref. ) . 3. Dicloxcillin : Parentral sol. Stable for 7 days at RT ( 14 day if ref. ). 4. Cloxacillin : Parentral sol. Stable for 14 days ( ref. ) . 5- Flucloxacillin : Parentral sol. Stable for 7 days ( ref. ) Storage : Store between 15 – 30oC
References : • Web site e.g. www. .com . • Drug Information Handbook 12th Edition 2004 – 2005 pages ( 452 , 642 , 1062 , 1137 ). • USP DI Edition 1999 , pages ( 2251, 2252, 2253, 2254, 2255, 2256, 2262 ) . • Principle of Medicinal Chemistry 4th Edition page 778-779 .
Temocillin is a beta-lactamase-stable penicillin with a selective. Gram-negative spectrum of activity and a long half-life The urinary excretion by 12 h was 70.58% of the administered