Download
1 / 26
260 likes | 962 Views
What is sIgA?. Principal immunoglobulinHumoral element in secretory immune systemHas a neutralizing component to prevent attachment and adherence of oral bacteriaSIgA adheres selectively to M cells in intestinal Peyer's patches, thus mediating the transepithelial transport of the Ab molecule from the intestinal lumen to underlying gut-associated organized lymphoid tissue.

E N D
1. Paul T. Rose et al
Pediatric Dentistry: July/August 1994
Volume 16, Number 4
http://www.aapd.org/upload/articles/rose-16-04.pdf IgA Antibodies to Streptococcus mutans in caries-resistant and -susceptible children
2. Principal immunoglobulin isotype in the body�s external secretions, main humoral element of the secretory immune system. IgA neutralizes viruses, bacterial exotoxins, and enzymes that contribute to disease processes and inhibit the attachment and adherence of oral bacteria to epithelial and tooth surfaces.
An important activity of mucosal surfaces is the production of Ab referred to as secretory IgA (SIgA). SIgA serves as the first line of defense against microorganisms through a mechanism called immune exclusion. In addition, SIgA adheres selectively to M cells in intestinal Peyer�s patches, thus mediating the transepithelial transport of the Ab molecule from the intestinal lumen to underlying gut-associated organized lymphoid tissue. In Peyer�s patches, SIgA binds and is internalized by dendritic cells in the subepithelial dome region. When used as carrier for Ags in oral immunization, SIgA induces mucosal and systemic responses associated with production of anti-inflammatory cytokines and limits activation of dendritic cells. In terms of humoral immunity at mucosal surfaces, SIgA appears thus to combine properties of a neutralizing agent (immune exclusion) and of a mucosal immunopotentiator inducing effector immune responses in a noninflammatory context favorable to preserve local homeostasis of the gastrointestinal tract.
In humans, Peyers� patches are described as macroscopic lymphoid aggregates that can be seen by the naked eye in the serosal side of the small intestine, with the greatest density found in the ileumPrincipal immunoglobulin isotype in the body�s external secretions, main humoral element of the secretory immune system. IgA neutralizes viruses, bacterial exotoxins, and enzymes that contribute to disease processes and inhibit the attachment and adherence of oral bacteria to epithelial and tooth surfaces.
An important activity of mucosal surfaces is the production of Ab referred to as secretory IgA (SIgA). SIgA serves as the first line of defense against microorganisms through a mechanism called immune exclusion. In addition, SIgA adheres selectively to M cells in intestinal Peyer�s patches, thus mediating the transepithelial transport of the Ab molecule from the intestinal lumen to underlying gut-associated organized lymphoid tissue. In Peyer�s patches, SIgA binds and is internalized by dendritic cells in the subepithelial dome region. When used as carrier for Ags in oral immunization, SIgA induces mucosal and systemic responses associated with production of anti-inflammatory cytokines and limits activation of dendritic cells. In terms of humoral immunity at mucosal surfaces, SIgA appears thus to combine properties of a neutralizing agent (immune exclusion) and of a mucosal immunopotentiator inducing effector immune responses in a noninflammatory context favorable to preserve local homeostasis of the gastrointestinal tract.
In humans, Peyers� patches are described as macroscopic lymphoid aggregates that can be seen by the naked eye in the serosal side of the small intestine, with the greatest density found in the ileum
3. Goal of Study Compare levels of IgA1 and IgA2 antibodies to saliva
Quantify S.mutans in caries-resistant (CR) and caries-susceptible (CS) children
Analyze sIgA and IgA1 and IgA2 subclass levels in whole and parotid using ELISA.
IgA1made by bone marrow B cells
IgA2 made by B cells in mucosa IgA1 is found in serum and made by bone marrow B cells.
In IgA2, the heavy and light chains are not linked with disulfide but with noncovalent bonds. IgA2 is made by B cells located in the mucosa and has been found to secrete into colostrum, maternal milk, tears and saliva.
IgA1 is found in serum and made by bone marrow B cells.
In IgA2, the heavy and light chains are not linked with disulfide but with noncovalent bonds. IgA2 is made by B cells located in the mucosa and has been found to secrete into colostrum, maternal milk, tears and saliva.
4. Methods Random selection
Fluoridated communities
Min of 20 subjects per group
21 CR (DMFS less than or equal to 1)
20 CS (DMFS greater than 5)
B/w 7-11 yrs of age
Negative PMH
No meds
Mixed dentition w/ 6�s, 1�s, 2�s
Consent Random selection from the dept of pediatric dentistry at Indiana University School of DentistryRandom selection from the dept of pediatric dentistry at Indiana University School of Dentistry
5. Saliva sampling One clinician collected samples to reduce variability b/w 8am-noon for unstimulated parotid and whole saliva
Whole saliva samples
Parotid saliva samples
Unstim saliva samples were diluted 1:10 and 1:100 in sterile saline and spiral plated in duplicate on mitis salivarius (MSS) agar supplemented w/15% sucrose and bacitracin for enumeration of total oral streptococci and S.mutans.
S.mutans was quantified from whole saliva by colonial morphology and incubated for 3 days and the % of S. mutans per total oral streptococci was calculated
Whole saliva samples were taken by patients expectorating into a test tube for 5 min.
Parotid saliva samples were taken by a suction cup apparatus placed over the parotid duct for 20 min to collect unstim parotid saliva.
A portion was used immediately to count m.o.s. and the rest was frozen at -20 C and used later for immunoglobulin and antibody analyses.Whole saliva samples were taken by patients expectorating into a test tube for 5 min.
Parotid saliva samples were taken by a suction cup apparatus placed over the parotid duct for 20 min to collect unstim parotid saliva.
A portion was used immediately to count m.o.s. and the rest was frozen at -20 C and used later for immunoglobulin and antibody analyses.
6. ELISA sandwich and direct techniques were used to determine concentrations of whole salivary total IgA, IgA1, IgA2 and parotid salivary total IgA.
The direct detection method originated in the 1940s when Coons and colleagues labeled antibodies with a fluorescent tag to mark tissue antigens. In this technique, a labeled primary antibody reacts directly with the antigen.
Results analyzed by student�s t-test
P values greater than 0.05 were significant
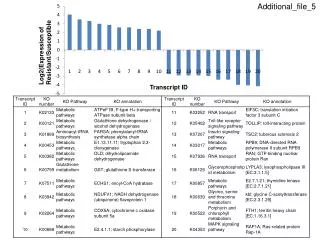
7. This study was designed to examine the total oral streptococci and S.mutans numbers for each child and divide the S.mutans numbers by the streptococcal numbers to calculate the proportion of S.mutans for each sample.
No significant differences b/w CR and CS groups were found in regards to the levels of parotid salivary IgA antibody to S.mutans, the levels of whole salivary IgA1 antibody to S.mutans, or the levels of whole salivary IgA1 antibody to S.mutans, or the levels of whole salivary IgA2 antibody to S.mutans.
However, there were significantly greater levels of whole salivary IgA antibody to S.mutans in the CR than in the CS children.
POINT: Whole salivary IgA in CR was greater than CS.This study was designed to examine the total oral streptococci and S.mutans numbers for each child and divide the S.mutans numbers by the streptococcal numbers to calculate the proportion of S.mutans for each sample.
No significant differences b/w CR and CS groups were found in regards to the levels of parotid salivary IgA antibody to S.mutans, the levels of whole salivary IgA1 antibody to S.mutans, or the levels of whole salivary IgA1 antibody to S.mutans, or the levels of whole salivary IgA2 antibody to S.mutans.
However, there were significantly greater levels of whole salivary IgA antibody to S.mutans in the CR than in the CS children.
POINT: Whole salivary IgA in CR was greater than CS.
8. Antibody activity proportions to the total immunoglobulin concentrations were calculated. There was no difference in proportions of parotid salivary IgA antibody to S.mutans/total parotid salivary IgA b/w CR and CS children.
POINT: CR individuals had a greater proportion of whole salivary IgA antibody to S.mutans/total whole salivary IgA than CS childrenAntibody activity proportions to the total immunoglobulin concentrations were calculated. There was no difference in proportions of parotid salivary IgA antibody to S.mutans/total parotid salivary IgA b/w CR and CS children.
POINT: CR individuals had a greater proportion of whole salivary IgA antibody to S.mutans/total whole salivary IgA than CS children
9. Key Points Individual differences in flow rate and IgA antibody content for each subject were considered, there was a significant difference b/w CR and CS individuals for IgA antibodies to S. mutans in whole saliva.
# of salivary S.mutans higher in CS than CR children
IgA antibodies levels to S.mutans in whole saliva was higher in CR than CS children.
Explanation: the difference in whole saliva but not in parotid saliva is that the greater numbers of S.mutans in whole saliva of CS children may absorb a greater amount of whole salivary IgA antibody to S.mutans than the lower S.mutans numbers in CR saliva.
Explanation 2: CR children produce a greater amount of sIgA antibody to S.mutans in minor, submandibular, sublingual salivary glands than CS children.Explanation: the difference in whole saliva but not in parotid saliva is that the greater numbers of S.mutans in whole saliva of CS children may absorb a greater amount of whole salivary IgA antibody to S.mutans than the lower S.mutans numbers in CR saliva.
Explanation 2: CR children produce a greater amount of sIgA antibody to S.mutans in minor, submandibular, sublingual salivary glands than CS children.
10. Main Fxn of IgA IgA functions at three anatomical levels in relation to mucosal epithelium: 1) luminal SIgA Ab prevents adhesion and entry of Ag into the epithelium; 2) IgA Ab in the lamina propria binds and excretes Ag to the lumen; and 3) IgA Ab in transit through the epithelium can inhibit virus production or neutralize proinflammatory Ags . An additional property of IgA is its inability to trigger the release of inflammatory mediators through receptors specific for its Fc domain (http://www.jimmunol.org/cgi/content/full/178/1/27)
11. Lawrence A.Tabak, DDS, PhD
Pediatric Dentistry � 28:2 2006
http://www.aapd.org/upload/articles/tabak-28-2.pdf In Defense of the Oral Cavity: The Protective Role of the Salivary Secretions
12. The secret is in the whole Analyzed salivary proteins assigned them to a protein family
Each individualized molecule plays a role
Protein roles:
Adhesins
Agglutinins
Antimicrobial
pH modulating Adhesions, if they supported bacterial attachment to hydroxyapatite
Agglutinitins: if they could clump bacteria or viruses (lysozyme, mucins, and salivary agglutinin, subsequently identified as lung scavenger receptor cysteine � rich protein gp-340
Antimicrobial: if they could slow or put a stop to bacterial growth (histatins, lactoferrin, peroxidase, lysozyme, among others)
pH modulating: if they could raise plaque pHAdhesions, if they supported bacterial attachment to hydroxyapatite
Agglutinitins: if they could clump bacteria or viruses (lysozyme, mucins, and salivary agglutinin, subsequently identified as lung scavenger receptor cysteine � rich protein gp-340
Antimicrobial: if they could slow or put a stop to bacterial growth (histatins, lactoferrin, peroxidase, lysozyme, among others)
pH modulating: if they could raise plaque pH
13. Current view of salivary function Alimentation: giving or receiving of nourishment
Tissue coating: saliva lubricates and hydrates soft tissues, these attributes are derived from mucin-glycoprotein content. 2 species were purified from human saliva. MG1 and MG2. MG2 is the gene product of MUC7, whereas MG1 is a mix of gene products MUC5B, MUC4, and MUC19. Each polypeptide is an array of carbohydrate side chains � oligosaccharides, which impart much of the unique properties of this class of molecule.Alimentation: giving or receiving of nourishment
Tissue coating: saliva lubricates and hydrates soft tissues, these attributes are derived from mucin-glycoprotein content. 2 species were purified from human saliva. MG1 and MG2. MG2 is the gene product of MUC7, whereas MG1 is a mix of gene products MUC5B, MUC4, and MUC19. Each polypeptide is an array of carbohydrate side chains � oligosaccharides, which impart much of the unique properties of this class of molecule.
14. Saliva in Children At Birth, IgA not detectable
4-6 wks levels rapidly rise
IgA1 dominates, by 20 wks IgA2 increases to adult levels.
Early childhood: lysozyme and salivary peroxidase are at adult levels
MUC5B dominates over MUC7 from 1mo-1yr
Antimicrobial peptides:
Beta-defensin-3
Cathelicidin LL37
Alpha-defensins 1,2,3
HNP1-3 were greater in cavity free children
More work is needed to understand he innate immune system of the oral cavityMore work is needed to understand he innate immune system of the oral cavity
15. http://www.sciencedaily.com/releases/2005/02/ "The eyes may be the window to the soul, but many scientists would say the mouth is the window to the body" �Science Daily
16. Saliva and other oral fluids contain many of the same proteins and molecules as blood and urine do.
Saliva can reveal disease, i.e. cancer
Developing technology for identifying molecules �biomarkers� for disease
Determines who vulnerable pt is to caries
�-human�s sugar chain makeup (oligosaccharides) is 100% genetically determined and cannot be changed. The USC researchers found that the sugar chain makeup in saliva can predict a child�s future cavity history to plus or minus one cavity with greater than 98% confidence�. Detect saliva proteins that have special sugars that bind to the surfaces of microbes. Various combos make people more or less prone to cavities. The combo�s of sugars doesn�t change much over time and preliminary research suggests that the test will be able to tell whether someone is likely to get cavities in his or her molars, premolars, or throughout the mouth.
More momentum on this research due to RNA molecules in saliva that can indicate whethere a patient has head and neck cancers, which is proof of principle that saliva testing can work for dx disease.
A further version of salivary testing can identify children with active tooth decay, which is important for public health implications in areas where families cannot afford routine dental care, and can help evaluate susceptibility and risk and the need for sealants and preventive measures.Detect saliva proteins that have special sugars that bind to the surfaces of microbes. Various combos make people more or less prone to cavities. The combo�s of sugars doesn�t change much over time and preliminary research suggests that the test will be able to tell whether someone is likely to get cavities in his or her molars, premolars, or throughout the mouth.
More momentum on this research due to RNA molecules in saliva that can indicate whethere a patient has head and neck cancers, which is proof of principle that saliva testing can work for dx disease.
A further version of salivary testing can identify children with active tooth decay, which is important for public health implications in areas where families cannot afford routine dental care, and can help evaluate susceptibility and risk and the need for sealants and preventive measures.
17. Gcamerica.com Saliva testing: good practice, good sense!Saliva-Check Buffer Kit
18. Patient Education Saliva neutralizes acid challenges, acts as a lubricant, forming pellicle on tooth surface and delivering calcium, phosphate, and fluoride.Saliva neutralizes acid challenges, acts as a lubricant, forming pellicle on tooth surface and delivering calcium, phosphate, and fluoride.
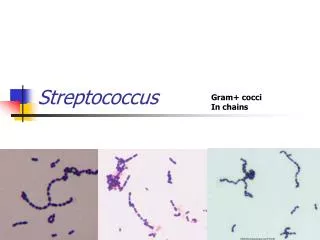
19. Patient Education Carbs and acidic foods amplify S.mutans and S.sobrinus in dental plaque which are related to the initiation and progression of dental caries.
20. Patient Education Once the salivary problem is identified the practitioner can recommend a course of preventive care (i.e. fluoride, chlorhexidine), lifestyle changes, altering oral hygiene, increasing saliva production.
21. 10 min of testing: Step 1:
Hydration
The rate of production of resting saliva as a surrogate measure of hydration. Pt sitting up and relaxed and gently grasp hold of the lower lip and to blot it gently with a qauze square. The time taken to form droplets of saliva on the minor glands of the lower lip can then be timed. Max time is 6 seconds.Pt sitting up and relaxed and gently grasp hold of the lower lip and to blot it gently with a qauze square. The time taken to form droplets of saliva on the minor glands of the lower lip can then be timed. Max time is 6 seconds.
22. 2. Consistency The viscosity of resting saliva as a surrogate for measuring its relative water and mucin content. Pt expectorates all resting saliva from their mouth into a small disposable cup. The second stage is to assess the viscosity of this saliva which can be determined by visual examination, watery, bubbly, frothy, and sticky.Pt expectorates all resting saliva from their mouth into a small disposable cup. The second stage is to assess the viscosity of this saliva which can be determined by visual examination, watery, bubbly, frothy, and sticky.
23. 3. Resting saliva pH The pH of resting saliva Tsi is done by dipping pH test paper directly into the sample of oral fluid to wet it, and then removing it immediately.Tsi is done by dipping pH test paper directly into the sample of oral fluid to wet it, and then removing it immediately.
24. 4. Stimulated saliva flow (5 min) The rate of production of stimulated saliva The pH paper is designed to function like a series of traffic lights, going from red through to yellow through to green. The colour is matched directly to the scale provided. This step tests for the quality of stimulated saliva in order to screen for the possibility of salivary gland disease, particularly gland damage from lymphocytic sialodenitis which can occur with a range of different medical conditions. To stimulate prodn of saliva, an inert piece of paraffin wax is typically used. Pt chews on wax and all saliva produced is drained into a cup. The volume measured is the liquid component and must be read at the bottom of the meniscus. From this value, one can then calculate the actual flow rate in ml/min, which is the recorded and classified using the traffic light system into very low, low, or normal. A normal individual produces 1ml of saliva per min when chewing.The pH paper is designed to function like a series of traffic lights, going from red through to yellow through to green. The colour is matched directly to the scale provided. This step tests for the quality of stimulated saliva in order to screen for the possibility of salivary gland disease, particularly gland damage from lymphocytic sialodenitis which can occur with a range of different medical conditions. To stimulate prodn of saliva, an inert piece of paraffin wax is typically used. Pt chews on wax and all saliva produced is drained into a cup. The volume measured is the liquid component and must be read at the bottom of the meniscus. From this value, one can then calculate the actual flow rate in ml/min, which is the recorded and classified using the traffic light system into very low, low, or normal. A normal individual produces 1ml of saliva per min when chewing.
25. 5. Stimulated saliva pH Higher concentration of bicarbonate ions in parotid saliva and should be a higher pH than the resting pH.
26. 6. Buffering capacity Buffering capacity of stimulated saliva in an aqueous env w/ differing amts of lactic acid. A small pipette is used to withdraw a small quantity of saliva, which is placed on test pads. Low buffer capacity � bright red (0pts)
Normal buffer � green (4pts)
Intermediate buffer � blue (2pts)
12 pt scale is created to keep track of any changes in buffer capacity over time.
Score b/w 10-12 is normal capacity
The remaining sample can be used for immuno-assay for S. mutans levels.