Download
1 / 52
520 likes | 767 Views
Scope of the Problem. 20 million (10.8%) with CKD

E N D
1. Evolving Concepts in the Treatment of the Patient with CHF and CKD Scope of the problem
Stage 3-4 CKD
ACE inhibitors
Diuretics
Ultrafiltration
ESRD
ACE inihibition
b blockers
Ultrafiltration
Transplantation
2. Scope of the Problem 20 million (10.8%) with CKD � 8 million with stage 3 or 4 CKD
400,000 (0.1%) with ESRD
Incidence of CHF 1/100 over age of 65
CKD increases all cause mortality in CHF
Worsening renal function in CHF predicts hospital death and complications
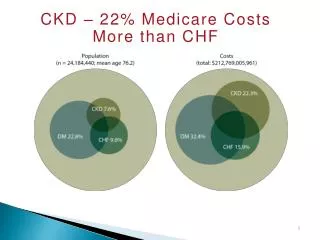
3. Prevalence of CHF in Prevalent Patients Point Prevalent General Medicare (age 66 & older) & ESRD Patients
5. Impact of Worsening Renal Function (WRF) Among Patients Hospitalized with Heart Failure (JACC 43:61-67, 2004) 1,004 consecutive patients with CHF
WRF ( Scr > 0.3 mg/dL) occurred in 27%
Risk factors � history of CHF, DM, Scr > 1.5 mg/dL, SBP > 160 mmHg
WRF increased risk of:
Complications � ARR 2.1
Hospitalization > 10 days � ARR 3.2
Hospital death � ARR 7.5
6. Case 1 A 70 y/o man with a 20-year history of Type II diabetes, a 7-year history of coronary artery disease (E.F. 25%), and diabetic nephropathy (Baseline creatinine 2.8 mg/dl) was admitted because the serum creatinine increased to 4.5 mg/dl after institution of lisinopril at a dose of 5 mg/dl. Medication on admission consisted of Glyburide 10 mg qd, Imdur 60 mg/qd, aspirin 81 mg qd, lisinopril 5 mg qd, and Lasix 80 mg qd.
Physical examination revealed BP 102/50 mmHg, pulse 81, bilateral rales, S3 gallop, ascites and 3+ bilateral lower extremity edema.
Labs � Na/K = 133/5.1, Cl/HCO3 = 101/17
BUN 76, creatinine 4.6
Duplex ultrasound � Widely patent renal arteries
7. The ACE inhibitor is discontinued. Over the next 3 days, the creatinine decreases to 3.8 mg/dl, his weight increases 2 kg, and he develops increasing dyspnea. A cardiology consultant recommends reinstitution of the ACE inhibitor for afterload reduction. To ameliorate this patient�s signs and symptoms of fluid overload, you should:
A) add hydralazine
B) intensify the diuretic regimen
C) resume the ACE inhibitor
D) perform isolated hemofiltration
8. Case 2 A 22 y/o woman with ESRD due to sickle cell nephropathy and a dilated cardiomyopathy (E.F. 20%) is admitted with fluid overload (10 kg above dry weight). Her interdialytic weight gains average 4.6 kg.
Physical examination reveals BP 123/71, pulse 96, weight 59 kg, bilateral pleural effusions, S3 gallop, ascites, and 2+ lower extremity edema.
An echocardiogram shows global hypokinesis with an E. F. of 20% but no pericardial effusion.
9. The house staff requests a cardiology consult who recommends institution of an ACE inhibitor. You should:
A) begin an ACE inhibitor
B) hemofiltrate the patient to her dry weight over several days
C) begin hydrazaline for afterload reduction
D) never call a cardiologist for a case like this
10. ACEI and Angiotensin II Antagonism in CHF
11. Influence of Renal Function on the Hemodynamic and Clinical Responses to Long-term Captopril Therapy in Severe Chronic Heart Failure 101 patients NYHA IV
Stratified according to serum creatinine (Scr):
Group I � Scr <1.4 mg/dL
Group II � Scr 1.4-2.8 mg/dL
Group III � Scr > 2.8
Captopril 1 to 3 months
Hemodynamic and clinical assessment baseline and after ACEI
(Packer et al, Ann. Intern. Med. 104:147-154 1986)
13. Clinical Benefit of ACEI Improvement of at least 1 NYHA functional class
Related to pretreatment renal function (p < 0.005):
Group I � 29/40 (73%)
Group II � 29/49 (59%)
Group III � 2/12 (17%)
14. ACEI in Older Patients with Heart Failure and Renal Dysfunction Prospective cohort study 10 community hospitals
1,076 patients discharged with diagnosis of CHF
Follow up for 6 months
Abnormal renal function � Scr > 2.0 mg/dL
(Philbin et al., J. Am. Geriatr. Soc. 47:302-08, 1999)
15. Baseline Characteristics
16. Severity Adjusted Clinical Outcomes
17. The Association Among Renal Insufficiency, Pharmacotherapy and Outcomes in Patients with CHF and Coronary Disease (Ezekowitz et al. JACC 44:1587-92, 2004) Prospective cohort study
6427 patients with CHF and CAD
One-year follow-up
39% with creatinine clearance < 60 ml/min
Outcome � one-year mortality
20. Renal Insufficiency and Heart Failure (McAlister et al. Circulation 109:1004-09, 2004) Prospective cohort study
754 patients
2.5-year median follow-up
56% with creatinine clearance < 60 ml/min
Outcome � survival one year
21. Potential Adverse Effects of ACEI in Patients with CHF and CKD Hyperkalemia
Hypotension may limit fluid removal with diuretics
Acute on chronic renal failure
Older age
Diuretic use
Decrease in MAP
28. Diuretic Therapy Diuretic therapy improves signs and symptoms of CHF
Chronic diuretic therapy decreases afterload and increases C.O.
Intravenous diuretics:
Improve signs and symptoms of CHF
Neurohormonal activation
Increase risk of AKI (? cardiorenal syndrome)
29. Effect of Diuresis on Cardiac Function, Weight, and Fluid Volumes in 6 Patients with Congestive Heart Failure
31. High-dose Furosemide Versus Low-dose Dopamine in the Treatment of Refractory CHF (Cotter et al. Clin. Pharmacol. Ther. 62:187-93, 1997) Randomized prospective trial
20 patients with refractory CHF:
Group A � Dopamine (4 mcg/kg/min) plus oral furosemide (80 mg/day)
Group B � Dopamine plus continuous IV furosemide (5 mg/kg/day)
Group C � Continuous IV furosemide (10 mg/kg/day)
72-hour follow-up
32. Results
35. Ultrafiltration Improved neurohormonal profile compared with IV diuretics
Greater weight loss and fluid removal
Significant decrease in 90-day morbidity
37. Ultrafiltration Versus IV Diuretics for Acute Decompensated CHF(Costanzo et al. JACC 49:675-83, 2007) Prospective randomized trial
200 patients with CHF and fluid overload: Ultrafiltration up to 500 ml/hr or IV diuretics � at least twice previous oral dose
Excluded � ACS, creatinine > 3.0, SBP < 90, Hct > 45, pressors
38. Results
40. CHF in ESRD 40-50% of patients with ESRD have CHF-mostly diastolic
Limited data with respect to efficacy of ACEI/ARB or b blocker therapy
Ultrafiltration mainstay of therapy
Renal transplantation improves LVEF
41. Prescription Patterns for Systolic Dysfunction Among Hemodialysis Patients(Roy et al. Am. J. Kid. Dis. 48:645-651, 2006) Prospective cohort study
420 patients � 11% with LVEF < 40%
Questionnaire regarding use/nonuse of ACEI or b blockers
42. Results 47 patients with EF < 40%:
b blocker � 72%
ACEI � 36%
Both � 26%
Reasons for not prescribing � concern regarding:
Adverse reactions � 88%
Adequate control with UF � 38%
Unproven benefit � 25%
Unfavorable risk/benefit � 17%
43. ACEI/ARB Therapy in ESRD Limited data
Efrati et al (Am. J. Kid. Dis. 40:1023, 2002)
Retrospective study
ACEI � 60 patients, no ACEI � 66 patients
52% decrease in cardiovascular mortality
Takahashi et al. (NDT 21:2507, 2006)
Randomized trial
Candesartan 4-8 mg � 43 patients, control � 37 patients
19-month follow-up
CVEs and CV death significantly higher in control group
44. Carvedilol Increases Survival in Dialysis Patients with Dilated Cardiomyopathy (JACC 41:1438, 2003) Prospective placebo � controlled trial
114 patients with:
NYHA class II or III CHF
LVEF < 35%
ACEI � 97%
Two-year follow-up
Primary endpoints � change in LVEDV, LVESV, LVEF
Secondary endpoints � all cause mortality, CVEs
47. Results
49. Improvement in �Uremic� Cardiomyopathy by Persistent Ultrafiltration(Toz et al. Hemodialysis Int. 11:46, 2007) Prospective study � 20-120 days
12 patients with C/T > 0.54 and LVEF < 45%
Dialysis regimen:
3 times/week, 4-5 hours
No antihypertensive agents
Isolated UF or post HD UF
Results � weight loss � 12 kg, C/T 0.59-0.47
51. Effect of Kidney Transplantation on LV Systolic Dysfunction and CHF in Patients with ESRD(Wali et al. JACC 45:1051, 2005) Observational cohort study
103 recipients with EF <40% - MUGA
6 and 12 months and last follow-up
Results:
LVEF 32 to 55%
70% achieved EF > 50%
15% remained with EF <40%
52. Summary In stage 3-4 CKD and Chronic CHF:
ACEI of limited hemodynamic and clinical benefit
Loop-blocking diuretics decrease afterload, improve LV function and are a cornerstone of therapy
In stage 3-4 CKD with acute decompensated CHF:
IV diuretics can have a negative hemodynamic and neurohumoral impact
Ultrafiltration should be considered as an alternative
In patients with ESRD:
Few data regarding the utility of ACEI/ARBs/b blockers
Persistent ultrafiltration or transplantation clearly beneficial