Download
1 / 10
110 likes | 430 Views
Management of Hyperglycemia in the Adult Hospitalized Patient. TEAM MEMBERS: Physicians: Maryann Emanuele, William Barron, Fadi Nabhan and Stephanie Painter Nurses: Rita Vercruysse MPH, Terse Bertucci APN/CNP,CDE

E N D
Management of Hyperglycemia in the Adult Hospitalized Patient TEAM MEMBERS: Physicians: Maryann Emanuele, William Barron, Fadi Nabhan and Stephanie Painter Nurses: Rita Vercruysse MPH, Terse Bertucci APN/CNP,CDE Donna Murphy APN/CNS,CDE, Theresa Pavone MSN, Barb Rumick CCRN, Barb Pudelek,ACNP, Rose Lach PhD, Pam Clementi, MSN, Camille Robinson (EPIC), Diabetes Liaisons Pharmacists: Barb Murphy and Alison Schriever Dietician: Jill Whitney RD/LD Center for Clinical Effectiveness: Michael Wall PharmD, Sr. Clinical Quality Improvement Analyst and Jan Jandristis Multidisciplinary ICU Committee
PLAN • Project Aim Statement: Create a consistent state of the art evidenced based approach to achieve normal blood glucose levels and standardize the management of hyperglycemia in hospitalized patients. • Measurement Goal and Target: Implemented insulin protocols to achieve tight glycemic control: ICU 80-120mgdL; Patient care units less than 110mg/dL pre prandial and random less than 180mg/dL. (7/04) No increased episodes of hypoglycemia.
DO Solutions Implemented: • Reviewed scientific literature and established a multidisciplinary ICU committee and consensus for insulin protocols and guidelines. • Developed protocols and guidelines for Intravenous Insulin Infusion and Transition from IV to Subcutaneous Insulin in Adult Patient. 10/03-12/03 - Protocols implemented. 4/04 • Initiated hospital wide nursing and physician education for protocols and the Basal Bolus insulin concept. 12/03 • Implemented protocol changes based on medical staff feedback and clinical outcomes. 7/04 & 9/04 • Changed nursing practice by adjusting blood glucose levels before meals and adjusting the prandial dose based on post meals. 7/04
DO Solutions Implemented: • Changed Food and Nutrition practice, ordering evening snacks for patients on the insulin protocols were not routinely ordered. • Implemented Non-ICU Hyperglycemia Insulin Therapy in Adults Patients who are eating. 9/04 • Removed sliding scale regular insulin from LUCI for better physiologic hyperglycemia control. 10/04 • Formed a Diabetes QI Steering committee 1/05 and unit based nurse “Train the Trainer” program. 5/05 • Developed RN and MD fact sheets on insulin protocols. 10/05 • Changed hypoglycemia treatment targets from 60mg//dL to 70mg/dL. • Added A1c lab order to all insulin protocols for patients with an admission glucose above 180mg/dL if not drawn in the last month. 11/05
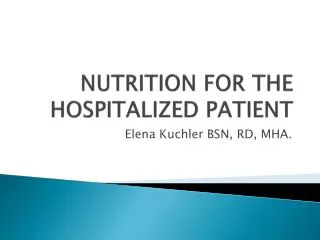
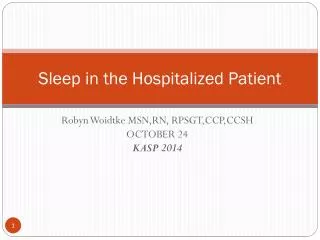
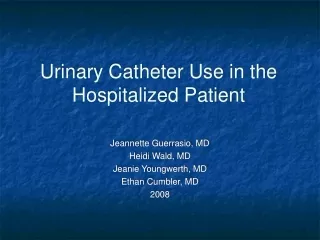
STUDY Analysis: • Graph 1: The control chart indicates a statistically significant improvement change in blood glucose levels beginning in 2004. Beginning in July 2004, there is a statistical significance at 99.7% (3 standard deviations) as compared to period prior to the insulin protocols. 2/03 through 3/04 • Graph 2: The median inpatient glucose value, which was previously stable with a median of 158mgd/L, has decreased and continues to decrease, with the implementation of inpatient insulin protocols. • Graph 3: The percent of inpatients with diabetes who experienced a day of hypoglycemia is not stable, the mean went from 10.43% to 11.74 % with the implementation of the insulin protocols. • Graph 4: The incidence of rescue therapy in patients receiving insulin has increased since 2003.
MEDIAN INPATIENT GLUCOSE UCL = 163.54 160 Mean = 156.79 155 UCL = 151.72 LCL = 150.03 150 Glucose (mg/dL) 145 Mean = 142.93 140 135 LCL = 134.15 04/2003 n=(8696) 09/2003 n=(9667) 11/2003 n=(9368) 12/2003 n=(9686) 02/2005 n=(8702) 04/2005 n=(9044) 05/2005 n=(9541) 06/2005 n=(8490) 07/2005 n=(8357) 10/2005 n=(8921) 11/2005 n=(9774) 01/2006 n=(9572) 02/2006 n=(4044) 02/2003 n=(10075) 03/2003 n=(11843) 05/2003 n=(10097) 06/2003 n=(10798) 07/2003 n=(11428) 08/2003 n=(11247) 10/2003 n=(11303) 01/2004 n=(11160) 02/2004 n=(11169) 03/2004 n=(11664) 04/2004 n=(11205) 05/2004 n=(12951) 06/2004 n=(11580) 07/2004 n=(11625) 08/2004 n=(10543) 09/2004 n=(11296) 10/2004 n=(11574) 11/2004 n=(11130) 12/2004 n=(12078) 01/2005 n=(11246) 03/2005 n=(11868) 08/2005 n=(11776) 09/2005 n=(10822) 12/2005 n=(12110) Month of Glucose Result (number of results) These data are confidential and to be used for quality improvement purposes only. Transition from IV to SubQ protocol and ICU insulin infusion released into LUCI Non-ICU hyperglycemia management protocol released into LUCI EPIC Inpatient Go-live Definition: Median inpatient glucose levels in patients with diabetes. Glucose readings below 40mg/dL and above 400mg/dL were excluded. Data Source: Clarity database, FORCE database. Analysis: The median inpatient glucose value, which was previously stable with a median of 158mg/dL, has decreased, and continues to decrease, with the implementation of inpatient insulin protocols.
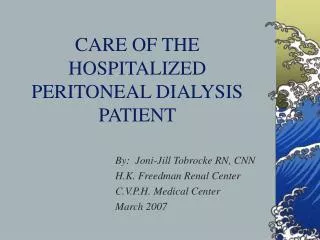
HYPERGLYCEMIA IN DIABETIC INPATIENTS 68 UCL = 67.60 66 Mean = 64.61 64 UCL = 63.48 62 LCL = 61.62 Mean = 60.25 Percent 60 58 LCL = 57.02 56 02/2003 (n=2149) 03/2003 (n=2525) 04/2003 (n=2005) 05/2003 (n=2278) 06/2003 (n=2296) 07/2003 (n=2452) 08/2003 (n=2321) 09/2003 (n=2155) 10/2003 (n=2405) 11/2003 (n=2066) 12/2003 (n=2162) 01/2004 (n=2545) 02/2004 (n=2369) 03/2004 (n=2523) 04/2004 (n=2450) 05/2004 (n=2625) 06/2004 (n=2395) 07/2004 (n=2345) 08/2004 (n=2069) 09/2004 (n=2174) 10/2004 (n=2267) 11/2004 (n=2118) 12/2004 (n=2248) 01/2005 (n=2236) 02/2005 (n=1859) 03/2005 (n=2114) 04/2005 (n=1893) 05/2005 (n=1844) 06/2005 (n=1494) 07/2005 (n=1727) 08/2005 (n=2132) 09/2005 (n=1999) 10/2005 (n=1863) 11/2005 (n=1850) 12/2005 (n=1874) 01/2006 (n=1755) Month (number of patient days) These information are confidential and to be used for quality improvement purposes only Transition from IV to SubQ protocol and ICU insulin infusion released into LUCI Non-ICU hyperglycemia management protocol released into LUCI EPIC Inpatient Go-live Definition: Number of diabetic inpatients who experience a day with a glucose measurement above 180mg/dL / Number of diabetic inpatient days with any glucose measurement. Glucose readings below 40mg/dL and above 400mg/dL were excluded. Data Source: Clarity database, FORCE database. Analysis: Hyperglycemia in inpatients with diabetes, which was previously unstable, has decreased, and continues to decrease, with the implementation of inpatient insulin protocols.
HYPOGLYCEMIA IN DIABETIC INPATIENTS 15 14 UCL = 13.87 13 UCL = 12.34 12 Mean = 11.74 Percent 11 Mean = 10.43 10 LCL = 9.61 9 LCL = 8.52 02/2003 (n=2149) 03/2003 (n=2525) 04/2003 (n=2005) 05/2003 (n=2278) 06/2003 (n=2296) 07/2003 (n=2452) 08/2003 (n=2321) 09/2003 (n=2155) 10/2003 (n=2405) 11/2003 (n=2066) 12/2003 (n=2162) 01/2004 (n=2545) 02/2004 (n=2369) 03/2004 (n=2523) 04/2004 (n=2450) 05/2004 (n=2625) 06/2004 (n=2395) 07/2004 (n=2345) 08/2004 (n=2069) 09/2004 (n=2174) 10/2004 (n=2267) 11/2004 (n=2118) 12/2004 (n=2248) 01/2005 (n=2236) 02/2005 (n=1859) 03/2005 (n=2114) 04/2005 (n=1893) 05/2005 (n=1844) 06/2005 (n=1494) 07/2005 (n=1727) 08/2005 (n=2132) 09/2005 (n=1999) 10/2005 (n=1863) 11/2005 (n=1850) 12/2005 (n=1874) 01/2006 (n=1755) Month (number of patient days) These information are confidential and to be used for quality improvement purposes only Transition from IV to SubQ protocol and ICU insulin infusion released into LUCI Non-ICU hyperglycemia management protocol released into LUCI EPIC Inpatient Go-live Definition: Number of diabetic inpatients who experience a day with a glucose measurement below 70mg/dL / Number of diabetic inpatient days with any glucose measurement. Glucose readings below 40mg/dL and above 400mg/dL were excluded. Data Source: Clarity database, FORCE database. Analysis: The percent of inpatients with diabetes who experience a day with a glucose measurement below 70mg/dL increased from 10.43-11.74% with the implementation of inpatient insulin protocols, and is not currently stable. Additional analyses are being performed to determine the source of the increased hypoglycemia.
USE OF RESCUE TREATMENT (glucagon or dextrose 50%) IN PATIENTS RECEIVING INSULIN 20 UCL = 19.59 18 16 Mean = 14.51 14 Percent of patients receiving rescue treatment following insulin 12 10 LCL = 9.43 02/2003 (354) 03/2003 (404) 04/2003 (348) 05/2003 (396) 06/2003 (356) 07/2003 (401) 08/2003 (402) 09/2003 (391) 10/2003 (402) 11/2003 (367) 12/2003 (398) 01/2004 (416) 02/2004 (382) 03/2004 (452) 04/2004 (447) 05/2004 (488) 06/2004 (509) 07/2004 (459) 08/2004 (462) 09/2004 (506) 10/2004 (456) 11/2004 (476) 12/2004 (492) 01/2005 (459) 02/2005 (452) 03/2005 (451) 04/2005 (449) 05/2005 (420) 06/2005 (395) 07/2005 (433) 08/2005 (453) 09/2005 (457) 10/2005 (451) 11/2005 (472) 12/2005 (472) Month (total patients receiving insulin) These data are confidential and to be used for quality improvement purposes only Transition from IV to SubQ protocol and ICU insulin infusion released into LUCI Non-ICU hyperglycemia management protocol released into LUCI EPIC Inpatient Go-live Definition: The percent of patients receiving rescue treatment (glucagon, dextrose 50%) following insulin therapy. Data Source: UHC Pharmacy database Analysis: The incidence of rescue therapy in patients receiving insulin has increased since 2003.
ACT Next Steps: • Develop Continuous Tube Feed Protocols. • Develop protocols for steroid use and protocols for cyclic tube feeds. • Mandate annual nursing competency test on e-learning for insulin protocols. • Develop nursing competency test on e-learning for hypoglycemia treatment. (2006) • Analyze cause for increase in hypoglycemia with the implementation of the insulin protocols. Consider treatment guidelines that address the severity of the hypoglycemia. • Monitor protocol effectiveness, staff compliance and protocol violations through outcome data collection. • Share protocol outcome data and experience in appropriate physician, nursing and pharmacy publications. • Plan an all day seminar on insulin protocols for Loyola staff and outside hospitals.