Download
1 / 25
270 likes | 853 Views
Pneumonia well explained from radiological point of view in detail

E N D
PNEUMONIA DR. BIJAY KUMAR YADAV 1ST YEAR RADIOLOGY RESIDENT I.K AKHUNBAEV KSMA, BISHKEK, KYRGYZSTAN
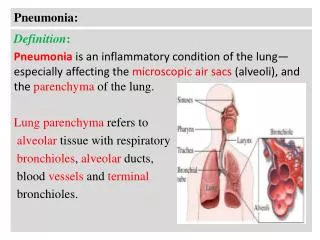
INTRODUCTION: • Pneumonia is an infection that inflames the air sacs in one or both lungs. The air sacs may fill with fluid or pus (purulent material), causing cough with phlegm or pus, fever, chills, and difficulty in breathing • Many organisms, including viruses and fungi, can cause pneumonia, but the most common causes are bacteria, in particular species of Streptococcus and Mycoplasma.
What ever are the cause, x-rays appearance look very much same, because x-rays appearances are so non-specific • No useful classification of pneumonia can be based on x-rays alone • Radiologist can draw most useful distinction between primary and secondary pneumonia • Major purpose of chest imaging: to establish whether or not pneumonia. • Basic radiological feature: one or more areas of consolidation varying from a small ill-defined shadow to a large shadow involving the whole of one or more lobes
CLASSIFICATION: Radiological classification: • Lobar Pneumonia • Bronchopneumonia • Interstitial pneumonia
1. LOBAR PNEUMONIA Referring to homogeneous consolidation of one or more lung lobes, often with associated pleural inflammation. Causes: • Streptococcus pneumoniae • Haemophilusinfluenzae • Moraxella catarrhalis. • Mycobacteriumtuberculosis Clinical Features: • Productivecough • Dyspnea/SOB • Malaise/Fatigue • Fevers –sweating/chills/rigors • Pleuritic chest pain • Nausea, vomiting or diarrhea
X-ray of Right Side Pneumonia RUL Consolidation RML Consolidation RLL Consolidation
Pneumococcal pneumonia, chest radiograph reveals a left lower lobe opacity with pleural effusion.
Klebsiella pneumonia - large cavity in right lower zone following cavitation of pneumonic consolidation.
Radiological signs: • Early stage: Lung markings get more and thicker in the suffered lobe or segment, or no X-ray findings. • Progressive stage: The radiograph shows consolidations localized to the affected lobe. Occasionally, the sign of Air bronchogram or a complication such as pleural effusion, abscess formation or emphysema can be found on the X-ray film. • Last stage: The radiograph shows patchy opaque shadows localized to the affected lobe.
PATHOLOGY 4 Pathological Phases Of Lobar Pneumonia • Congestion: This stage occurs within the first 24 hours of contracting pneumonia. Pulmonary capillaries dilated and serous fluid leaks out of capillaries into the alveoli. The patient develop fever with SOB and cough. • Red Hepatization:2-3 days after the congestion. That means the lung look like “RED LIVER”. The affected lobe is solid as the alveoli are full of RBCs, Neutrophils, desquamated epithelial cells and Fibrin instead of air, so there is no gaseous exchange in this lobe. The patient becomes breathless and hypoxic. The cough is associated with blood stained or rusty sputum.
Grey Hepatization:2-3 days after Red hepatization and is an avascular stage. The affected part look like “GREY LIVER”. The alveoli are full of Neutrophils and Dense fibrous strands. The patient cough up purulent sputum and remain breathless. • Resolution:Begins after 8-10 days (without antibiotics). Monocytes clear the inflammatory debris and normal air filled lung architecture is restored. Improvement of patient's conditions is noticed.
PATHOPHYSIOLOGY Infection to the lung (e.g bacteria, virus) ▼ Inflammatory response initiated ▼ Alveolar edema + exudate formation ▼ Alveoli & respiratory bronchioles fill with serous exudate, blood cells, fibrin, bacteria ▼ Consolidation of lung tissues
2. BRONCHOPNEUMONIA Refers to more patchy alveolar consolidation associated with bronchial & bronchiolar inflammation often affecting both lower lobes. Causes: Most common causes are: Haemophilus influenzae Staphylococcus aureus Clinical features: Fever - Cough - Mucus Shortness of breath Chest pain Tachypnea Sweating Headache Muscle aches
X-ray Features: • Increase in the size & number of Lung markings. • Small patchy alveolar consolidation distribute along lung markings. • Lesions are frequently found in both lower lung fields. • The hilarshadows may become larger. • Affected position: lobule of lung
In Right Middle & Lower lung fields, on Admission & after Recuperation OnAdmission After Recovery
3. INTERSTITIAL PNEUMONIA • It is a heterogeneous group of diffuse parenchymal lung diseases characterized by specific clinical, radiologic and pathologic features. • Involves the areas in between the alveoli. Causes: • Bacteria, viruses or fungi • Mycoplasma pneumoniae is the most common cause Clinical Features: Fever SOB Cough
X-ray Features: • A lung volume loss and a craniocaudal gradient of peripheral septal thickening, Bronchiectasis & Honeycombing • Peribronchovascular Infiltrate
Complications Of Pneumonia: • Pleural effusion, Empyema & Pleurisy • Lung abscess • Bacteremia & Septic shock • Respiratory Failure
Pneumonia due to covid-19 • Covid-19 is a disease caused by the novel corona virus • Early symptoms of covid-19 are: A fever, Dry cough & Shortness of breath • If your COVID-19 infection starts to cause pneumonia, you may notice things like: • Rapid heartbeat • Shortness of breath or breathlessness • Rapid breathing • Dizziness • Heavysweating
Chest CT Scan findings in Covid-19 Pneumonia Patient Chest CT scan from a 65-year-old man with COVID-19. Pneumonia caused by the new coronavirus can show up as distinctive hazy patches on the outer edges of the lungs, indicated by arrows. (ground glass opacities)