Nitric Oxide Therapy
Educative presentation for medical graduates and postgraduates


Nitric Oxide Therapy
E N D
Presentation Transcript
Nitric Oxide Therapy Dr CSN Vittal
Inhaled nitric oxide • Inhaled nitric oxide (iNO) is a pulmonary vasodilator that plays a major role in regulating vascular muscle tone. • It has emerged as a treatment for hypoxemic respiratory failure in newly born infants that is associated with persistent high pulmonary vascular pressure and resultant right-to-left shunting of blood (persistent pulmonary hypertension of the newborn)
Inhaled nitric oxide • Inhaled NO therapy is successful in treating ARDS because of its vasodilator properties. • It reduces pulmonary artery pressure and causes vasodilation of the blood vessels that supply the ventilated regions. Ignarro IJ, Buga GM, Wood KS, Byrns RE, Chaudhuri G (1987)Endothelium-derived relaxing factor produced and released from artery and vein is nitric oxide. Proc Natl Acad Sci U S A. 84:9265–9269.
iNO vs ECMO • The Neonatal Inhaled Nitric Oxide Study Group trial documented that iNO reduced the need for ECMO Neonatal Inhaled Nitric Oxide Study Group (NINOS) (1997) Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure. N Engl J Med 336:597–604.
History • 1980 : Furchgott and Zadawaski, - proposed acetylcholine stimulated the formation of a substance in the endothelial cell that subsequently caused smooth muscle relaxation- “endothelial-derived relaxing factor” (EDRF) • 1987 – Ignarro et al, showed that EDRF and NO have identical properties • 1992 – Roberts et al & Kinselet al report success of NO in babies with PPHN
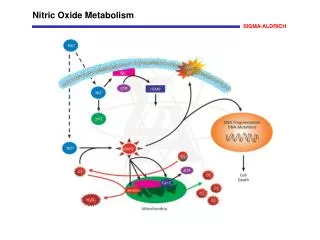
Properties of NO • Colorless, odorless hydrophobic free radical • Half life : 3-5 sec • Diffuses freely through cell membranes • Rapidly metabolized to nitrite and nitrate • Synthesized from arginine via nitric oxide synthetase (NOS) • Inactivated in blood by binding to Hgb, forming methemoglobin
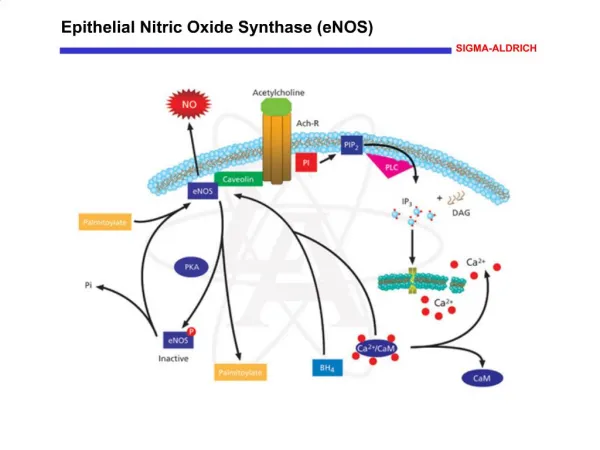
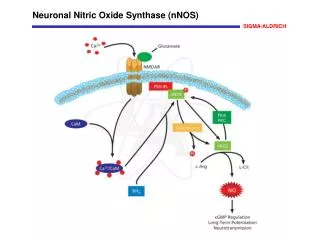
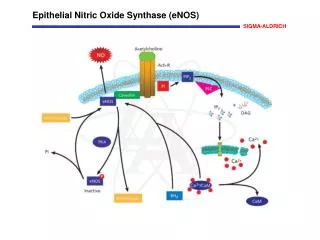
Nitric Oxide Synthetase (NOS) • 3 isoforms, all use L-arginase as substrate • Endothelial • Neuronal • Inducible • Responsible for basal vasomotor tone • Activated by Ca++ influx • Produces NO in picomolor quantities • Stimulated by Ach, bradykinin, ATP, shear stress
Action of NO on smooth muscle • Within smooth muscle, NO binds to the heme moiety of soluble guanylate cyclase • This generates cGMP from GTP • cGMP activates protein kinases which dephosphorylate myosin light chains, preventing myosin-actin interactions • cGMP also decrease in intracellular CA++ and increase permeability of the K+ channel, leading to hyper-polarization of the cell membranes Both mechanisms lead to vasodialatation
Other Actions of NO • Potent platelet inhibitor • Decreased adhesion • Increased disaggregation • Inhibition of vascular smooth muscle cell proliferation • Immunomodulation • Gene toxicity • Inhibits Endothelin release
Persistent Pulmonary Hypertension of Newborn • Foetal circulation is marked by high degree of pulmonary vasoconstriction • Failure of postnatal drop of PVR or development of elevated PVR leads to R to L shunting at the foramen ovale or ductus arteriosus • Management includes • hyperoxygenation, • hyperventilation, • alkalosis, • systemic BP support and • nonspecific vasodilators
PPHN - Pathophysiology • Elevated circulating and endothelial cellular entothelin (ET) • Some have vascular smooth muscle proliferation • Hypoxia increase ET release and inhibit NO release • ? Decreased NOS activity • ? L-arginine deficiency
iNO in PPHN- Protocol • Indications • Term or near term (>34 weeks) • Evidence of PPHN • Optimal pre-NO management • A-a DO2/OI : 550-600 for 1 hour OR • OI > 20 for 2 hours OR > 25 for 1 hour
pre-NO management • ‘Open-lung’ ventilation • Mild hypocarbia/alkalosis • Good systemic BP • Volume • Pressors • Surfactant if indicated • Sedation + paralysis
Oxygenation Status • A-a DO2 : [FiO2 X (Patm – 47) – (1.25 X PCO2)] • Oxygenation Index [MAP X FiO2 X 100 / PaO2] • A-a Gradient (at sea level) • Age 20 years: 4 to 17 mmHg • Age 40 years: 10 to 24 mmHg • Age 60 years: 17 to 31 mmHg • Age 80 years: 25 to 38 mmHg values: very good < 5, medium 10 - 20, poor > 25
NO Protocol • Initiate iNO at 20 ppm • ABG in 2—30 min • Response = > 2-% improvement in PaCO2 • If no response: wean off iNO • If response, maintain iNO for 6-12 hours
NO Protocol - Monitoring • ABG q4-6 hrs • Check methemoglobin at 8 and then every 24 hours • DecreaeiNO if metHb > 5 % • Continuous monitoring of NO2 • Decrease iNO if NO2 > 5 ppm • Clninical bleeding
Weaning • After 6-12 hours, begin FiO2 and ventilator weaning • When FiO2 < 0.60, wean iNO • Wean by 5 ppm every hour until dose is 5 ppm, then wean in hourly steps of 1 ppm • If deteriorates, go back to previous step, wait for 4 hours
NO – Other Uses • COPD: • NO therapy in COPD is to preserve lung function by maintaining adequate gas exchange. • Pulsed delivery of combined NO and oxygen may maximize the potential benefit of this form of therapy in patients with COPD. • ARDS: • Inhaled NO therapy is successful in treating ARDS because of its vasodilator properties. • It reduces pulmonary artery pressure and causes vasodilation of the blood vessels that supply the ventilated regions.
Methemoglobin • NO is absorbed into the blood where its binds to the ion of the heme protein, subsequently producing nitrosylhemoglobin, which is oxidized to methemoglobin with the release of nitrates. Methemoglobin levels should be measured frequently and kept <2.5%
Conclusions Inhaled NO therapy is an effective form of treatment in acute conditions, such as ARDS and PPHN; it is particularly effective in increasing oxygen saturation and decreasing pulmonary artery pressure. It also seems to be effective in chronic disorders, such as COPD and pulmonary hypertension.