Download
1 / 39
400 likes | 790 Views
Changes in Health-Related Quality of Life in Older Women after Diagnosis with Gynecologic Cancer. Amy Klapheke, MPH, PhD Public Health Institute, Cancer Registry of Greater California NAACCR/IACR Combined Annual Conference June 11, 2019. Outline. Background Methods Results Discussion.

E N D
Changes in Health-Related Quality of Life in Older Women after Diagnosis with Gynecologic Cancer Amy Klapheke, MPH, PhD Public Health Institute, Cancer Registry of Greater California NAACCR/IACR Combined Annual Conference June 11, 2019
Outline • Background • Methods • Results • Discussion
Gynecologic Cancer in Older Women • Older women at increased risk of gynecologic tumors • Serious impact on physical and mental wellbeing • Adverse treatment side effects • Disease-related symptoms • Psychological problems • Coexisting chronic conditions • Improvements in treatment and survival focus on improving quality of life
Health-Related Quality of Life (HRQOL) • Multi-dimensional concept that indicates the impact that health status has on quality of life • Physical, social, emotional, mental, functional well-being of a person • Valuable in cancer research • Give patient perspective • Assess symptom prevalence and severity • Develop effective treatment and care plans • Evaluate impact and benefit of treatment
Study Objectives • Existing research is limited • Older women underrepresented • Lack pre-cancer diagnosis data • Purpose: • To evaluate the impact of gynecologic cancer diagnosis in older women • Aims: • 1) To assess the likelihood of developing functional impairments in older women after gynecologic cancer diagnosis • 2) To estimate the pre- to post-diagnosis changes in HRQOL in these women compared to cancer-free controls
Surveillance, Epidemiology, and End-Results – Medicare Health Outcomes Survey (SEER-MHOS) • Links cancer registry data and survey data of Medicare Advantage enrollees • Includes demographic, clinical, treatment information and self-reported data about HRQOL • Presently includes 18 cohorts of MHOS data from 1998-2017, SEER cases through 1973-2015*
Surveillance, Epidemiology, and End Results (SEER) Program SEER registries included in SEER-MHOS
Medicare Health Outcomes Survey (MHOS) • Survey of Medicare Advantage beneficiaries • Used to monitor quality of care since 1998 • Each cohort: baseline survey + 2 year follow-up survey • Core questionnaire: demographics, socioeconomic data, comorbidities, activities of daily living, HRQOL
Study Population Cancer Cases • Female SEER-MHOS participants, 1998-2014 • >65 years old at time of survey • Resided in SEER region • Cases • First primary invasive cervical, ovarian, or uterine cancer • Cancer diagnosis between baseline and follow-up survey • Controls • No cancer • Completed a baseline and follow-up survey Cancer-Free Controls
Aim 1 Outcomes • Measure of functional impairment: activities of daily living (ADLs)1 • Difficulty eating, bathing, dressing, getting in/out of chairs, using the toilet, walking • Depressive symptoms • Based on algorithm2 using questions from the Diagnostic Interview Schedule in MHOS 1S. Katz, Assessing self-maintenance: activities of daily living, mobility, and instrumental activities of daily living, J. Am. Geriatr. Soc. 31 (1983) 721–727. 2K. Rost, M.A. Burnam, G.R. Smith, Development of screeners for depressive disorders and substance disorder history, Med. Care. 31 (1993) 189–200.
Aim 2 Outcomes • HRQOL in SEER-MHOS • 1998-2005: Medical Outcomes Study Short Form-36 (SF-36) • 2006-2014: Veteran-RAND 12-Item Health Survey (VR-12) • 8 domains summarized into: • Physical component summary (PCS) scores • Mental component summary (MCS) scores • Algorithm used to normalize scores to general population • Scale of 0-100 (mean + SD = 50 + 10)
Statistical Analysis • Propensity-score matched 5:1 • Chi-square tests: comparisons by cancer status • Multiple logistic regression: odds of functional impairments and depressive symptoms at follow-up • Mixed effects linear models: estimate changes in scores between baseline and follow-up
Statistical Analysis • Propensity-score matched 5:1 • Chi-square tests: comparisons by cancer status • Multiple logistic regression: odds of functional impairments and depressive symptoms at follow-up • Mixed effects linear models: estimate changes in scores between baseline and follow-up
Statistical Analysis • Propensity-score matched 5:1 • Chi-square tests: comparisons by cancer status • Multiple logistic regression: odds of functional impairments and depressive symptoms at follow-up • Mixed effects linear models: estimate changes in scores between baseline and follow-up
Statistical Analysis • Propensity-score matched 5:1 • Chi-square tests: comparisons by cancer status • Multiple logistic regression: odds of functional impairments and depressive symptoms at follow-up • Mixed effects linear models: estimate changes in scores between baseline and follow-up
Table 1. Characteristics of the study population (N =1,488). *Statistically significant at p<0.05
Table 1. Characteristics of the study population (N =1,488). *Statistically significant at p<0.05
Results: Aim 1 1) To assess the likelihood of developing functional impairments in older women after gynecologic cancer diagnosis
Table 2. Adjusted+ odds of functional impairments and depressive symptoms at follow-up in women with gynecologic cancer relative to cancer-free controls, stratified by stage at diagnosis.
Table 2. Adjusted+ odds of functional impairments and depressive symptoms at follow-up in women with gynecologic cancer relative to cancer-free controls, stratified by stage at diagnosis.
Table 3. Adjusted+ odds of functional impairments and depressive symptoms at follow-up in women with gynecologic cancer relative to cancer-free controls, stratified by time since diagnosis.
Table 3. Adjusted+ odds of functional impairments and depressive symptoms at follow-up in women with gynecologic cancer relative to cancer-free controls, stratified by time since diagnosis.
Results: Aim 2 • 2) To estimate the pre- to post-diagnosis changes in HRQOL in these women compared to cancer-free controls
Table 4. Adjusted+ least squares mean HRQOL scores at baseline and follow-up surveys in women with gynecologic cancer compared to cancer-free controls.
Table 4. Adjusted+ least squares mean HRQOL scores at baseline and follow-up surveys in women with gynecologic cancer compared to cancer-free controls.
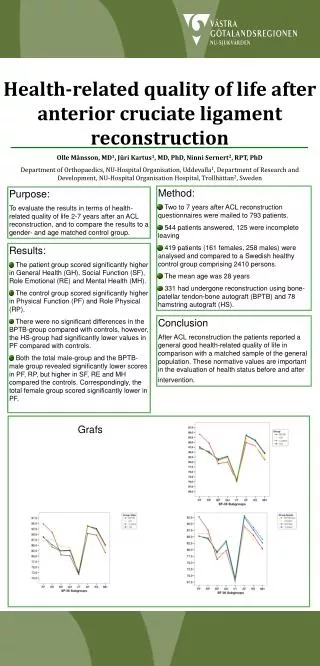
Figure 1. Adjusted+ mean changes in HRQOL scores between baseline and follow-up by stage at diagnosis in gynecologic cancer patients and controls.
Figure 1. Adjusted+ mean changes in HRQOL scores between baseline and follow-up by stage at diagnosis in gynecologic cancer patients and controls.
Figure 2. Adjusted+ mean changes in HRQOL scores between baseline and follow-up by time since diagnosis in gynecologic cancer patients and controls.
Summary • Older women with gynecologic cancer were significantly more likely to experience functional limitations and depressive symptoms than cancer-free women • Both physical and mental HRQOL significantly decreased after diagnosis with gynecologic cancer • Greatest in those with advanced disease • Worsening scores regardless of time since diagnosis • Results underscore need for interventions to reduce pain, provide support, and prepare patients for changes
Limitations and Strengths • Limitations • Sample size limited ability to assess sites separately • Did not account for treatment • Limited to Medicare managed care plan enrollees • Strengths • Longitudinal • Comparison to matched controls • Valid and reliable measures of HRQOL • Pre-cancer diagnosis data
Implications • Quantifies the effects of gynecologic cancer on HRQOL • Provides a reference point for clinical trials and research • Can be used to design targeted interventions to enhance quality of life and prolong meaningful survival
Acknowledgments • Rosemary Cress, DrPH • Theresa Keegan, PhD MS • Rachel Ruskin, MD • Colleagues at Public Health Institute, Cancer Registry of Greater California
Thank you! Contact: Amy Klapheke, MPH, PhD Public Health Institute Cancer Registry of Greater California Sacramento, CA aklapheke@crgc-cancer.org 916-779-0279