Download
1 / 23
260 likes | 1.16k Views
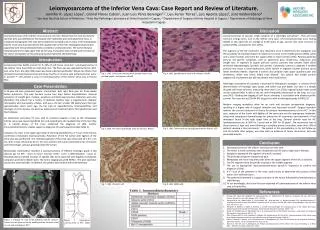
ACP Case Presentation: LEIOMYOSARCOMA OF THE INFERIOR VENA CAVA – DIAGNOSTIC AND THERAPEUTIC CHALLENGES. Prasanth Reddy MD; Department of Internal Medicine Peter J. VanVeldhuizen MD; Division of Hematology/Oncology; Department of Internal Medicine University of Kansas – Kansas City

E N D
ACP Case Presentation:LEIOMYOSARCOMA OF THE INFERIOR VENA CAVA – DIAGNOSTIC AND THERAPEUTIC CHALLENGES Prasanth Reddy MD; Department of Internal Medicine Peter J. VanVeldhuizen MD; Division of Hematology/Oncology; Department of Internal Medicine University of Kansas – Kansas City September 10, 2004
Case Presentation • 68 year old female • Chief complaint – progressive dyspnea over two years • Initial Evaluation prior to transfer – “Normal” • Sleep study • Nocturnal hypoxia • Echocardiogram • Right atrial mass
Case Presentation • Past Medical History: • Hypertension • Peripheral neuropathy of feet • Interstitial cystitis • Hysterectomy • Social History: • Remote tobacco use • Family History: • Coronary artery disease • Gastric cancer • Stroke • Diabetes Mellitus
Physical Exam • Vital signs • Temperature 378 • Blood pressure 104/76 • Pulse 100 • Respirations 18 • Oxygen saturation 90% on room air • Not tachypneic or cyanotic • Lungs – normal • Cardiovascular – normal • Extremities – trace pedal edema
Differential diagnosis • Thrombus • Myxoma • Sarcoma • Metastatic disease
A B CT Chest Panel A - Large mass in the inferior vena cava. Panel B - Tumor mass within the right atrium.
A B MRA/MRI Panel A - Large mass centered at the confluence of the inferior vena cava and right atrium, extending into the right atrium. Panel B - Mass extending beneath the diaphragm.
Further Evaluation - Negative CT Head CT Abdomen/Pelvis V/Q Scan Doppler US bilateral lower extremities
A B H&E Desmin Pathology Panel A: H&E stain showing spindle cells. Panel B: Tumor is positive for desmin (brown) indicating smooth muscle lineage consistent with leiomyosarcoma.
Operative Findings • Origin • Posterior aspect of the IVC • Dimensions • 8 x 4 cm • Procedure • Excision of mass and adherent IVC • Closure of Patent Foramen Ovale (PFO)
Leiomyosarcoma of the inferior vena cava • Malignant tumor of vascular origin 1 • About 200 cases reported worldwide 2 • Metastatic disease – <50% of cases 3,4 • Liver, Lung, Lymph nodes, Bone • Sixth decade 5 • Female predominance 5 1 Brewster DC, et al. Arch Surg. 1976 Oct;111(10):1081-5. 2 Lee SW, et al. Korean J Gastroenterol. 2003 Sep;42(3):249-54. 3 Cacoub P, et al. Medicine (Baltimore). 1991 Sep;70(5):293-306. 4 Griffin AS, et al. J Surg Oncol. 1987 Jan;34(1):53-60. 5 Hemant D, et al. Australas Radiol. 2001 Nov;45(4):448-51.
Clinical Findings • Non-specific clinical findings 6 • Dyspnea • Malaise • Weight loss • Abdominal or back pain • Symptoms may precede diagnosis by several years 6 6 Gowda RM, et al. Angiology. 2004 Mar-Apr;55(2):213-6.
Clinical Findings • Manifestations dependent upon the location of the tumor 3 • Segment I - Palpable mass • Segment II - Abdominal pain • Segment III - Variants of Budd-Chiari syndrome 3 Cacoub P, et al. Medicine (Baltimore). 1991 Sep;70(5):293-306.
Pathology • Biopsy required for diagnosis • Histopathology 7 • Spindle tumor cells • Positive for markers of smooth muscle activity • Desmin • Vimentin • Muscle actin • Alpha-smooth muscle actin 7 Nikaido T, et al. Pathol Int. 2004 Apr;54(4):256-60.
Diagnostic Modalities • Imaging modalities 5 • Echocardiography • CT • MRI • PET • PET/CT • First reported use of PET/CT that assisted in the diagnosis of leiomyosarcoma of the inferior vena cava 5 Hemant D, et al. Australas Radiol. 2001 Nov;45(4):448-51.
Management • Not adequately described 8 • Limited international experience • “Optimal management unknown” 8 Hines OJ, et al. Cancer. 1999 Mar 1;85(5):1077-83.
Management • Aggressive surgical treatment is recommended 4 • Slow growth pattern • Relatively low metastatic potential • Complete resection 9 • feasible • associated with improved survival • Chemotherapy and radiation therapy may serve as adjuncts 8 4 Griffin AS, et al. J Surg Oncol. 1987 Jan;34(1):53-60. 8 Hines OJ, et al. Cancer. 1999 Mar 1;85(5):1077-83. 9 Hollenbeck ST, et al. J Am Coll Surg. 2003 Oct;197(4):575-9.
Prognosis • Case series from Memorial Sloan-Kettering 9 • 25 patients • Complete resection • 3-year survival rate - 76% • 5-year survival rate - 33% • Incomplete resection - No 3-year survivors 9 Hollenbeck ST, et al. J Am Coll Surg. 2003 Oct;197(4):575-9.
Prognosis • Main prognostic factor – “topography” 3 • Highest level of extension of the tumor • Upper-segment tumors - poorest prognosis • Overall prognosis 10 • Poor • Mean survival of around 2 years 3 Cacoub P, et al. Medicine (Baltimore). 1991 Sep;70(5):293-306. 10 Bendayan P, et al. Ann Chir. 1991;45(2):149-54.
Leiomyosarcoma of the inferior vena cava • Rare malignant tumor • smooth muscle cells of the media • Diagnosis challenging • non-specific complaints - dyspnea, malaise, weight loss, and abdominal or back pain • Various imaging modalities assist diagnosis • echocardiography, CT, MRI, PET, and PET/CT • make earlier diagnosis possible • Aggressive surgical management combined with adjuvant therapy
Acknowledgements • Gregory F. Muehlebach, MD; Division of Cardiovascular Surgery, Department of Surgery, University of Kansas School of Medicine, Kansas City, KS. • David G. Meyers, MD, MPH; Division of Cardiology, Department of Internal Medicine, University of Kansas School of Medicine, Kansas City, KS. • James P. Birkbeck, MD; Division of Cardiology, Department ofInternal Medicine, University of Kansas School of Medicine, Kansas City, KS. • Stephen K. Williamson, MD; Division of Hematology/Oncology, Department ofInternal Medicine, University of Kansas School of Medicine, Kansas City, KS. • Peter J. VanVeldhuizen, MD; Division of Hematology/Oncology, Department ofInternal Medicine, University of Kansas School of Medicine, Kansas City, KS.