Download
1 / 21
260 likes | 961 Views
USE OF CALCIUM PHOSPHATE BONE CEMENT FOR FRACTURE FIXATIONS IN OSTEOPOROTIC PATIENTS. By: Sindhu Gowri. Agenda. Bone Composition Osteoporosis Market Analysis Bone Replacement Options Calcium Phosphate bone cement Manufacturing method Fracture Fixations Clinical Trials

E N D
USE OF CALCIUM PHOSPHATE BONE CEMENT FOR FRACTURE FIXATIONS IN OSTEOPOROTIC PATIENTS By: Sindhu Gowri
Agenda • Bone Composition • Osteoporosis • Market Analysis • Bone Replacement Options • Calcium Phosphate bone cement • Manufacturing method • Fracture Fixations • Clinical Trials • Future Directions
Bone composition • Bone is the main support system of the body. • It is a dynamic tissue which is replaced everyday in our lives. • Bone is made up of minerals such as calcium, phosphorous, sodium, potassium, chloride, fluoride etc. • The calcium content in bone is 34.8 wt%, and in hydroxyapatite is 39.6 wt%. • Other important substances found in the human bone are water (8- 10 wt %), and collagen (35 wt %).
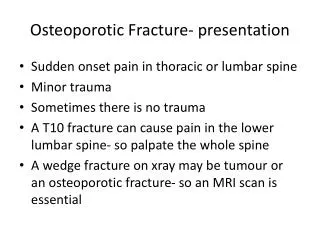
Osteoporosis • “A skeletal disorder characterized by compromised bone strength (bone density and bone quality) predisposing to an increased risk of fracture” – WHO • Factors: age, gender, family history, diet and exercise. • Measurement and Prediction: Bone Mineral Density (BMD) • T-score value: if the BMD is <-2.5 SD.
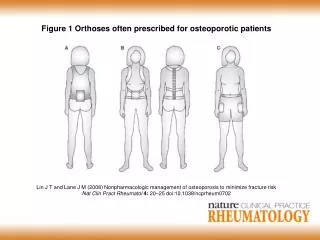
Osteoporosis…cont Weak and porous structure: • The decrease in the bone mass. • Imbalance in the production and usage of calcium, therefore the bone voids are not filled in completely. • This leads to instability in fixing metal hardware such as bone screws and plates resulting in poor performance of the implants. Source: Bone and Joint Decade http://www.boneandjointdecade.org/eLecture/1609/GMaalouf.html
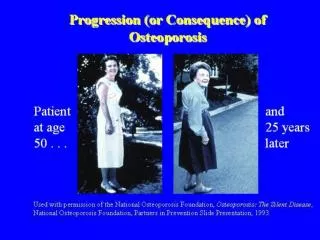
Osteoporosis in women • Osteoporosis is gender related. • In women after menopause estrogen level decreases resulting in decreased production of minerals and bone. • Women at the age of 35 are at the peak BMD. • BMD decreases significantly during menopause (1-5 % decrease in bone mass) • Further decrease leads to osteoporosis. http://imaginis.com/osteoporosis/osteo_diagnose.asp
Market Analysis (U.S) • Currently there are 2 million fractures annually due to osteoporosis in the U.S. • The estimated medical care costs for osteoporotic patients is 14 billion $. • By 2050 the expected medical care costs for osteoporotic fractures would go up to $ 25 Billion and the number of fractures expected would be greater than 3 million. • Approximately there are 300,000 surgeries which use calcium phosphate bone cement for fracture fixation in the U.S annually • This constitutes to a revenue of anywhere between $ 10 million to 1.5 billion annually
Mechanics of Fracture • Fractures could be due to • Bending • Torsion • Both are a combination of tension and compression on different planes. • Torsion results in a spiral fracture at an angle of 45 degrees. • Bone is strongest in compression, weaker in tension and weakest in shear.
Bone Replacement Options • Autografts: • Among 100 patients atleast 20 of them experience surgical morbidity. • Allografts: • Clinical trails have shown the risk of transmitted HIV. • PMMA: • Thermal necrosis • Bioinert
Calcium Phosphate Cement • Is capable of hardening into calcium deficient hydroxyapatite and remodeling at a similar rate to bone (1-2 years). • Different forms: monocalcium phosphate monohydrate, dicalcium phosphate dihydrate, hydroxyapatite, and alpha and beta tricalcium phosphate (TCP). • Although beta phase tricalcium phosphate is very biocompatible, it does not form calcium deficient hydroxyapatite (CDHA) in the body. • This is the reason why alpha TCP is preferred to be used as bone void fillers.
Manufacturing method of alpha-TCP • Calcium carbonate (CaCO3) and Calcium pyrophosphate (Ca2P2O7) are mixed thoroughly using a ball mill. • After it is mixed, it is heated to a temperature of 13000 C at a rate of 40 C per minute using a furnace. • The composition is degassed at every 300, 800 and 11000 C. After degassing is done, the milled TCP is removed and immediately quenched in air. CaCO3 + Ca2P2O7 ------- Ca3 (PO4)2 + CO2 (g) • Alpha-TCP is now mixed with SiO2 by heating up to a temperature of 1325 degree C and rapid quenching in air.
Preparation methods • Both the cement and the liquid (sodium silicate) are unloaded from the plastic vials. • The cement is mixed using a mortar and a pestle at the operating room temperature right before injection. • It is mixed for a minute until a paste is obtained (shear application). • The mixed cement paste is then transferred from the mortar to a sterile syringe (5cc-10cc) using a hard spatula. • Once injected into the body, the cement cures and hardens within twelve hours.
Fracture Fixation Source: Skeletalkinetics, CA
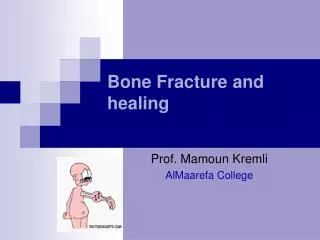
Bioactivity analysis • The liquid and powder (ratio of 0.34ml/g) undergoes a solid-state reaction at 370 C forming silicone induced calcium deficient hydroxyapatite (CDHA+Si). • New bone formation in silicone doped cement. • Osteoclasts are also seen in silicon doped cement (bone resorption). • Silicone has excellent osteoblastic activity, enhanced reactivity with collagen and apatite increasing the rate of bone remodeling.
Bioactivity analysis (2 weeks) Source: Camire C.L“Material Characterization and in vivo behavior of silicon substituted alpha-tricalcium phosphate cement,”
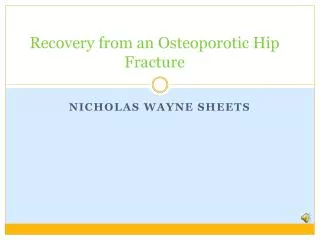
Cement Clinical Trials • Norian SRS, Cupertino, California • Clinical trials were done in the year 2000 on a total of 110 patients selected randomly. • 55 patients were treated with Norian SRS cement. A cast was also applied on the fracture for two weeks after the cement was injected into the voids. • The other 55 patients were treated with closed reduction method. Closed reduction was achieved using a cast and plates for six weeks.
Number of patients having pain at distal forearm according to the VAS in both groups
Future Directions • Clinical trial results: absence of infections, low immobilization and rest periods (2 weeks Vs 5 weeks), and most importantly less pain. • The next step for this cement would be to prove its ability in eradicating back pain through kyphoplasty. • Employment of vacuum mixing for better injectability. • Other future applications would be seen in sports medicine with the addition of BMPs and antibiotics into the cement.
References • Camire C.L, “Enhancing material and biological properties of calcium phosphate bone substitutes,” Thesis 2005, 2-10 (2005). • Schneider E., J. Goldhahn and P. Burckhardt, “The challenge-Fracture Treatment in Osteoporotic Bone,” Osteoporosis, Vol 16, S1-S2. (2005) • Larsson S., “Cement Augmentation in Fracture Treatment,”Scandinavian Journal of Surgery, Vol 95, No. 2, 111-118. (2006) • Larrisson S. and T.W. Bauer, “Use of injectable calcium phosphate cement for fracture fixation: a review,”Clinical Orthopaedics and Related Research, No. 395, 23-32. (2002) • C. T. Laurencin, Bone Graft Substitutes, (ASTM International, US 2003), pp. 3-15. • Elder S., E. Frankenburg, J. Goulet, D. Yetkinler, R. Poser and S. Goldstein, “Biomechanical Evaluation of Calcium Phosphate Cement-Augmented Fixation of Unstable Intertrochanteric Fractures,”Journal of Orthopaedic Trauma, Vol 14, No. 6, 386-393. (2000) • Camire C.L, S.J Saint-Jean, C. Mochales, P. Nevsten, J.S. Wang, L. Lidgren, I. McCarthy and M.P Ginebra, “Material Characterization and in vivo behavior of silicon substituted alpha-tricalcium phosphate cement,”Thesis 2005, Paper V, 1-9. (2005)