Download
1 / 96
1k likes | 1.23k Views
Everything You Need to Know About Geriatric Psychiatry in 75 Minutes. Andrea Stewart, MD, FRCPC Writer of LMCC, 2002. Aged ≥ 80 years in 1994 Aged ≥ 80 years in 2020. AGE DEPENDENCY RATIO. Proportion of population aged ≥ 80 years (%). Challenges of Late Life.

E N D
Everything You Need to Know About Geriatric Psychiatry in 75 Minutes Andrea Stewart, MD, FRCPC Writer of LMCC, 2002
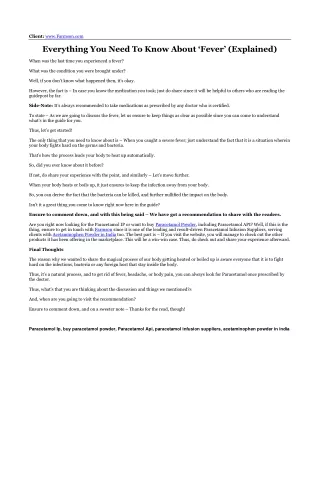
Aged ≥80 years in 1994Aged ≥80 years in 2020 AGE DEPENDENCY RATIO Proportion of population aged ≥80 years (%)
Challenges of Late Life • Co-morbid medical illness / cognitive disorders • Sensory loss • Financial worries • Retirement • Dependency • Dying and death • Bereavement
OVERVIEW • Dementia - BPSD • Late Onset Psychosis • Depression in late life • Anxiety in late life • Delirium • Other types of dementia (Lewy Body, FTD)
Approach to Memory Loss • Speaking to the person (safety first) • Speaking to the family (safety first) • History, physical examination • Create a differential and then direct investigations (bloodwork, urinalysis, ECG, imaging) to firm up the diagnosis • Investigations • Follow-up Plan
Differential Diagnosis • Delirium • Cognitive Impairment but not dementia/ Mild Cognitive Impairment/ Age Associated Memory Decline • Dementia - subtypes • Depression or other psychiatric illness • Other CNS disease (cancer, demyelination, etc.) or a dementia secondary to GMC
Alzheimer’s Dementia • Memory Impairment • One or more other cognitive impairment: • Aphasia, apraxia, agnosia, executive functioning deficit • Gradual onset and continual decline • Impairments cause significant social or occupational functional decline compared to previous level of functioning • Impairments are not delirium, substance-induced, or caused by another GMC or psychiatric illness
Defining the Diagnostic Threshold Normal Cognition MCI/ CIND Dementia
Screening Tools • MMSE score <24/30 • MOCA score <26/30 • Mini-Cog (3 word registration & recall, CDT)
Work-up1 • CBC, Cr, urea, electrolytes, TSH, vitamin B12 • Neuroimaging if the onset is recent (<1 year), early (<65), or the presentation is atypical or suggestive of another neurological disease • Other tests prn (VDRL, HIV, carotid U/S, EEG, chest Xray, urinalysis, LP) • ECG prior to medication management 1Burns A, BMJ
OBTAIN MEAL/SNACK KEEP APPOINTMENTS USE HOME APPLIANCES TELEPHONE FIND BELONGINGS MAINTAIN HOBBY DISPOSE LITTER CLEAR TABLE SELECT CLOTHES WALK EAT TRAVEL ALONE GROOM DRESS Bars show 25th to 75th %ile of patients losing independent performance. Activities of Daily Living 30 25 20 15 10 5 0 MMSE Mild AD Moderate AD Severe AD Adapted from Galasko. Eur J Neurol. 1998;5(suppl 4):S9-S17; Galasko et al. Alzheimer Dis Assoc Disord. 1997;11(suppl 2):S33-S39.
Cognitive Enhancers • May improve: • ADLs- activities of daily living, time to institutionalization • Behaviour/Mood- decreased concomitant psychotropics • Cognitive enhancement • Types • Acetylcholine-esterase inhibitors (boost ACh) • NMDA antagonists (Block glutamate)
Other Medications/ CAM • Nimodipine (Ca channel blocker) at 90 to 180 mg/day • General BP lowering • Vitamin B12 • Extract of Ginkgo biloba 761 • Vitamin E no longer used due to bleeding risk • DHEA may be harmful to memory • Cognitive training, reminiscence therapy
ABC Approach A Antecedents B Behaviours C Consequences
Physical: delirium, diseases, drugs, discomfort, disability • Intellectual: dementia – cognitive abilities/losses • Emotional: depression, psychosis • Capabilities: environment not too demanding yet stimulating enough, balancing demands and capabilities • Environment: noise, relocation, schedules… • Social, cultural, spiritual: life story, relationships family dynamics, personality traits... www.piecescanada.com
Pharmacological Management of BPSD • Atypical antipsychotics1 • RSP & OZP reduce aggression, RSP reduces psychosis • Higher risk CVEs, EPS, death • Antidepressants2,3 • db trials show CIT = RSP with fewer SEs • Trazodone has trend of effectiveness in FTD • Benzodiazepines 1Cochrane, 2008; 2Pollock, BG Am J Ger Psych; 3Cochrane, 2008
The following is NOT true of Alzheimer’s: • Insidious, gradual and progressive decline • Motor symptoms are absent until later in the disease • A dramatic presentation is not the same as an abrupt onset • Behavioural symptoms are often the most distressing symptom for families and caregivers • The ‘head turning sign’ refers to sexual disinhibition • Vascular events may co-occur and cause cognitive dysfunction
Psychosis in the Elderly1 • 4% in the community • 15% presenting to a geriatric medicine clinic • 10-38% of people in LTC (21% of new admissions to LTC) 1Holyrood S, Int J Ger Psych 1999
Approach • Speaking to the family (safety first) • Speaking to the person (safety first) • History, physical examination • Create a differential and then direct investigations (bloodwork, urinalysis, ECG, imaging) to firm up the diagnosis • Investigations • Follow-up Plan
Differential Diagnosis • Psychosis in People <45 • MDE or Mania • SZP/SZA/ delusional D/O • 2 GMC/subs • Delirium • Personality disorder • Psychosis in People >45 • Cognitive Disorders (delirium, dementia) • 2 GMC/ Subs • Psychotic Disorder (SZP, SZA, Del D/O) or paraphrenia • MDE, Mania
Outcomes and Associated Factors • Elderly with psychosis are more likely to have a history of psychosis, live in LTC, and have lower MMSE scores1 1Holyrood S, Int J Ger Psych 1999
Which of the following is not true in LLP? • Most paranoid disorders of old age are due to schizophrenia • More women develop late onset schizophrenia • With ageing, schizophrenia tends to give less severe positive symptoms • Patients with schizophrenia live 10-30 years less on average
Case 7 What is in your differential diagnosis? What kind of investigations would you order? Assuming you believe her to be depressed what would be your plan of treatment? Is there a reason for suggesting one antidepressant over another? Assuming she does not have any response to treatment after 3 weeks what would you do?
Approach to Mood Complaint • History (with collateral) and physical examination • Make the diagnosis considering the differential, assess severity (psychosis) and suicidality • Thorough medication review • Investigate causes (bloodwork, urinalysis, ECG, imaging) and remove promoting factors • Review past episodes and treatments
Differential Diagnosis • Depressive Disorder (dysthymia, MDE, BP with MDE, personality disorder) • Bereavement • Dementia • Delirium • Substance (drug of abuse, medication) or GMC
Epidemiology1 • Lifetime risk 11% • Incidence in the general population: 4%/ year • Incidence in people > 65: 1-3%/ year • Incidence in hospitalized people: 11% • Incidence in people in LTC: 12-22% 1Narrow WE, NIMH ECA prospective data
Diagnostic Criteria Mood depressed/irritable or anhedonia for > 2 weeks and 4/8: • Sleep change • Interests lost • Guilty or worthless feelings • Energy lost • Concentration impaired • Appetite changed/ wt change • Psychomotor symptoms • Suicidal or death-related thinking DSM-IV-TR
Late Life Depression CCSMH, Assessment and Treatment of Depression 2006
Subtypes • With or without psychosis, graded severity, recurrent or first episode, bipolar depression • Secondary to something else • Dysthymia • Co-morbid with dementia or substance abuse
MDE vs Grief • Grief • Onset after death of loved one • Symptoms improve with time • Passive wishes to have died 1st or with person • Self esteem preserved • Sadness comes in waves • Functional impairment <2 mo. MDE • +/- onset after trigger • Symptoms worsen with time • SI/ preoccupation with death • Intense guilt & worthlessness • Persistent mood state • Functional impairment • Psychosis APA, 2000
Management • Mild: bibliotherapy, exercise, close follow-up or supportive therapy • Moderate: antidepressants +/- psychotherapy, or psychotherapy alone • Severe: refer to psychiatry, +/- hospitalization for safety, ECT, antipsychotics with antidepressants, psychotherapy alone only effective for specific patients if done by experts - otherwise in combination
Suicide Risk CCSMH, Assessment of Suicide Risk and Prevention of Suicide, 2006
Antidepressants • Meta-analysis of trials of 2nd generation antidepressants in people >60 with non-psychotic depression and no dementia 1American Journal of Geriatric Psychiatry, 2008
Antidepressant No change after 4wks Works >20% better Maintenance Go to 8 wks Reassess diagnosis, increase dose, switch to escitalopram, sertraline, mirtazapine, effexor >20% better after above: Li, antipsychotic, psychotherapy
Clinical Use of Antidepressants • If anything protective for suicide in elderly • Elderly more likely to die of overdose if taken • Electrolytes pre and post (1 week to 1 month) • Risk of GI bleed, especially with concurrent NSAID or ASA use - monitor, add gastroprotective agent • Follow q2 weeks for the first 1-3 months, keep on medication >1 yr post remission
Psychotherapy • Cognitive Behavioural Therapy • Problem Solving Therapy • Interpersonal Therapy