Download
1 / 98
1.04k likes | 1.56k Views
AUTACOIDS : Receptor- and Non Receptor-Mediated. Therapeutics 201, Learning Unit IV Semester 1, AY 2009-2010 Department of Pharmacology & Toxicology UP College of Medicine July 13, 2009. Autacoids : Agonists, Antagonists. Objectives: At the end of the session, students are expected to:

E N D
AUTACOIDS : Receptor- and Non Receptor-Mediated Therapeutics 201, Learning Unit IV Semester 1, AY 2009-2010 Department of Pharmacology & Toxicology UP College of Medicine July 13, 2009
Autacoids : Agonists, Antagonists Objectives: At the end of the session, students are expected to: • Review concepts pertaining to the inflammatory process • Define an autacoid • Describe the different autacoids in terms of (emphasis on histamine, serotonin, eicosanoids) • Distribution/site in the body • Synthesis/storage/release/metabolism • Factors that stimulate synthesis, release • Specific receptors • Pharmacologic action/effect of agonists, antagonists and enzyme inhibitors • Clinical applications
Concept MAP : Maintaining/Restoring Balance in Health/Disease
Clinical illness is produced by: Direct invasion of tissue Toxic compounds liberated by the organism The body’s response to the organism
The manifestations of disease are usually produced by various inflammatory mediators produced by: • the initiating organism or • the host • The resulting inflammation may be: • helpful in localising the causative infection or • harmful
Autacoids “Autacoids” : a varied group of endogenous substances occurring in minute amounts and possessing distinct chemical structure with distinct biologic/ pharmacologic activity Autos = self; Akos = medicinal agent or remedy (Greek).
AUTACOIDS • Naturally occurring substances • Localized in tissues • Do not normally circulate • Diverse physiological and pharmacological activities • Differ from hormones and neurotransmitters • Short duration of action • Usually involved in response to injury • Sites of action restricted to the synthesis area
Examples of autacoids • Amines: histamine, serotonin (5HT) • Polypeptides: kinins, oxytocin, angiotensin II, vasopressin, atrial natriuretic factor, endothelins. • Fatty acids: prostaglandins, leukotrienes, thromboxanes, platelet activating factor (PAF). • Others: endothelium-derived relaxing factor (NO), cytokines (proteins).
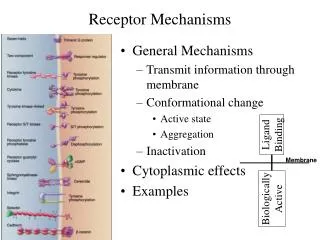
G-protein-coupled receptors (GPCRs)* • Major target of drug development • Signalling mechanism & potential target sites for drug action 1. Basal state (“switch off”) 2. Receptor-mediated GDP release 3. Subunit dissociation & effector regulation 4. Deactivation & return to basal state
Histamine (-aminoethylimidazole): a basic amine COOH Histamine is formed from histidine by histidine decarboxylase. Small amounts of histamine formed by bacteria in the gastro-intestinal tract (GIT) is broken down in the gut wall and liver.
Distribution of histamine • Widely distributed in: • - bacteria • - plants • - animals • - venoms and stinging fluids (stinging nettle, insect stings, bee venom).
Histamine • Signal involved in local immune response, also a neurotransmitter • synthesized by the decarboxylation of histidine • Either stored or quickly inactivated by histamine-N-methyltransferase and diamine oxidase • Release of histamine from mast cells is stimulated by IgE antibodies which respond to foreign antigens in the body
Synthesis • Decarboxylation of amino acid L-histidine catalyzed by pyridoxal PO4-dependent L-histidine decarboxylase. • Ingested from food or formed by bacteria in the GIT • Storage sites: • perivascular tissue – mast cell • circulation – basophil (bound to chondroitin SO4) • others – GIT, lungs, skin, heart, liver, neural tissue, reproductive mucosa, rapidly growing tissues and body fluids
Storage of histamine • ‘Slow-turnover’ histamine is stored as heparin-histamine complex in cytoplasmic granules in mast cells (lungs, GIT, skin) and basophils. • ‘Fast-turnover’ histamine is stored in CNS neurons, skin and enterochromaffin-like cells (ECL) of stomach.
Release of ‘Slow turnover’ histamine Allergic reaction: Antigen combines with IgE antibodies on the surface of mast cells or basophils. Mechanical–induced degranulation:e.g., scratch. Non-exocytotic:displacement of histamine from storage site by a drug, e.g., tubocurarine, morphine.
Histamine H1-receptors • Present in endothelium, smooth muscles cells, nerve endings. • Receptor activation → diacylglycerol and IP3 • Contract smooth muscles: intestine, bronchi • V/d: direct + NO release → flushing, headache • Vascular permeability : contract endothelial cells in venules) • Triple response: flush, flare and wheal. • Stimulate nerve endings: pain, itch; release epinephrine and norepinephrine from adrenal medulla; central excitation.
Pathophysiological action of histamine • Mediate type 1 hypersensitivity reactions: hives and hay fever. • Emesis: mediation of motion sickness • Histamine shock (hypotension): systemic anaphylaxis.
An Allergic Reaction • Early phase reaction: occurs within minutes of exposure to an allergen and lasts for 30-90 minutes • Late phase reaction: begins 4-8 hours later and can last for several days, often leading to chronic inflammatory disease
Symptoms • Allergic Rhinitis • Conjunctivitis • Bronchoconstriction • Urticaria • Atopic Dermatitis • Anaphylaxis http://allergy.healthcentersonline.com/nasalsinus/allergicrhinitis.cfm
Symptoms:anaphylaxis, swelling (skin, mucosa); itching, bronchospasm, hypotension, shock, phospholipase C and A2 activation. Liberators: large molecules (proteins – egg white, serum, venom, toxins); surface active agents, proteolytic enzymes, drugs etc. Clinical uses: diagnosis of achlorhydria, diagnosis of pheochromocytoma, and to verify integrity of axon reflexes.
Histamine H2-receptors Receptor activation: stimulation of adenylyl cyclase cAMP. • Parietal cells: H+ secretion. • Vascular smooth muscle cells: vasodilatation • Heart: force of contraction, HR.
Histamine H3-receptors • Largely presynaptic receptors in brain, myenteric plexus and other neurons. • Autoreceptors: negative feedback inhibition of histamine synthesis and release. • Heteroreceptor: release of norepinephrine, dopamine, serotonin and acetylcholine.
Histamine Antagonists • Physiologic antagonism – epinephrine • Release inhibitors – cromolyn sodium, Beta 2 adrenoceptor agonists • Histamine receptor antagonists
Histamine H1-receptor antagonists • Competitive; some are antimuscarinic, some block -adrenoceptors, and receptors for bradykinin, serotonin, and some have local anesthetic properties. • First generation antihistamines: lipid soluble → sedative (children may experience excitation) • Second generation antihistamines: Non-sedative: loratadine
First Generation Antihistamines • Small, lipophilic molecules that could cross the BBB • Not specific to the H1 receptor • Groups: • Ethylenediamines • Ethanolamines • Alkylamines • Piperazines • Tricyclics • Common structural features of classical antihistamine • 2 Aromatic rings • Connected to a central Carbon, Nitrogen or CO • Spacer between the central X and the amine • Usually 2-3 carbons in length • Linear, ring, branched, saturated or unsaturated • Amine is substituted with small alkyl groups eg CH3
Histamine Antagonists A.Ethanolamines • Carbinoxamine maleate • Clemastine fumarate • Diphenhydramine HCl • Dimenhydrinate B. Ethylenediamines • Pyrilamine maleate • Tripelennemine HCL/citrate • PPA C. Alkylamines • Chlorpheniramine maleate • Brompheniramine maleate First Generation Agents D. Piperazines 1. Hydroxyzine HCl/pamoate (long acting) 2. Cyclizine HCl/lactate 3. Meclizine HCl 4. Chlorcyclizine E. Phenothiazines 1. Promethazine HCl
Second Generation Antihistamines • Modifications of the First Generation Antihistamines to eliminate side effects resulted in the Second Generation Antihistamines • More selective for peripheral H1 receptors • Examples: • terfenadine • loratadine • cetirizine • mizolastine • astemizole
Second Generation Agents A. Alkylamines Acrivastine B. Piperazines Cetirizines HCl C. Piperidines Astemizole Levocabastine Loratadine Terfenadine Fexofenadine
“Next” Generation Antihistamines • Metabolite derivatives or active enantiomers of existing drugs • Safer, faster acting or more potent than Second Generation drugs • Examples: • Fexofenadine • Desloratadine • Levocetirizine
Therapeutic Uses: • Dermatosis • Allergic rhinitis • Motion sickness & emesis • Parkinson’s disease • EPS • Insomnia • Adverse reactions
Adverse Reactions and Side Effects • First Generation Drugs: • Anticholinergic CNS interactions • Gastrointestinal reactions • Common side effects: sedation, dizziness, tinnitus, blurred vision, euphoria, lack of coordination, anxiety, insomnia, tremor, nausea and vomiting, constipation, diarrhea, dry mouth, and dry cough • Second Generation Drugs: • Common side effects: drowsiness, fatigue, headache, nausea and dry mouth • Side effects are far less common in Second Generation drugs
Adverse Effects: • CNS : sedation, agitation, nervousness, delirium, tremors, incoordination, hallucinations, & convulsions - common in first generation antihistamines • GIT : vomiting, diarrhea, anorexia, nausea, epigastric distress, constipation - dryness of mouth, throat & airway, urinary retention - first generation • Headache, faintness • Chest tightness, palpitations, hypotension • Visual disturbances • Hematological - leukopenia, agranulocytosis, HA
Histamine H2-receptor antagonists • Competitive • Cimetidine, ranitidine, famotidine.
Uses of histamine H2-receptor antagonists • Secretion of H+ and pepsin: more effective on nocturnal (due to histamine) than food-induced (due to ACh, gastrin and histamine) secretion. - Gastric ulcer: normal H+, mucosal defense. - Duodenal ulcer: H+, Helicobacter pylori infection? - Reflux esophagitis - Zollinger-Ellison syndrome (gastrin producing tumor)
Side effects of histamine H2-receptor antagonists • Cimetidine (Tagamet) – antiandrogenic (gynecomastia in man), inhibit several cytochrome P450 drug metabolism pathways - hepatic [O] of many drugs (e.g., propranolol, alcohol). • Ranitidine (Zantac) – 5x more potent than cimetidine; reversible liver dysfunction. • Famotidine (Pepcid) – 5x more potent than ranitidine.
BIOGENIC AMINESSEROTONIN Source: plants (banana, pineapple, plums) & animals (mollusks, arthropods, mammals (platelets, not in mast cells). Biosynthesis: Hydroxylation of tryptophan, then decarboxylation to serotonin(5-hydroxy tryptamine;5-HT). Rapidly absorbed into secretory granules. Accumulated in platelets, degradation by oxidative deamination. Uses: No therapeutic use. Antagonists are highly useful.
Serotonin Synthesis 5-HT Precursor PCPA: inhibits TH