Download
1 / 25
250 likes | 482 Views
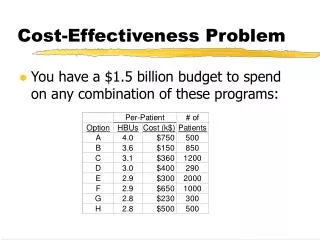
Background. High blood pressure contributes to a substantial amount of premature death and cardiovascular and renal diseases, and high intake of salt increases blood pressure.WHO set a worldwide target of a maximum salt intake of 5g/day, however, salt intake averaged about 9-12g/day around the world.The American Medical Association called for a 50% reduction in salt intake in the US in hopes of saving up to 150,000 lives annually..

E N D
1. Cost-effectiveness of Salt Reduction Interventions Darwin Labarthe, MD, MPH, PhD, Director
Guijing Wang, PhD, Senior Health Economist
Division for Heart Disease and Stroke Prevention
Centers for Disease Control and Prevention (CDC)
Atlanta, GA 30341, USA
2. Background High blood pressure contributes to a substantial amount of premature death and cardiovascular and renal diseases, and high intake of salt increases blood pressure.
WHO set a worldwide target of a maximum salt intake of 5g/day, however, salt intake averaged about 9-12g/day around the world.
The American Medical Association called for a 50% reduction in salt intake in the US in hopes of saving up to 150,000 lives annually.
3. Objectives To assess cost-effectiveness analyses of salt reduction interventions
To identify the main characteristics of this evidence
4. Concepts of economic evaluations Economics is about values, resources, and choices.
Maximize expected well-being subject to resource constraints.
Help policy or decision makers set resource allocation priorities.
5. Concepts of economic evaluations (cont) Cost-effectiveness analysis
Value the cost to improve a unit of health outcome by implementing an intervention program, usually compared with other programs.
Health outcomes measured in natural units such as life years gained or heart attack avoided.
6. Concepts of economic evaluations (cont) Two subtypes of cost-effectiveness analysis
Cost-utility analysis: health outcomes measured in quality-adjusted life years (QALYs) or other utility measures.
Cost-benefit analysis: health outcomes measured in monetary values.
7. Methods Literature search from databases
PubMed, EMBASE, EcoLit
Publications in English from January 2000 to May 2010
Search terms
Costs, cost-effectiveness, cost-utility, cost-benefit, or medical expenditure and sodium or salt reduction, intake, or consumption.
8. Literature search results 53 publications obtained from the search.
16 of them appear to be relevant cost-effectiveness studies based on titles and abstracts.
After careful review of the 16, 11 original research articles are relevant cost-effectiveness studies.
9. Literature search results (cont.) Among the 11 original research papers:
8 evaluated interventions in developed countries (high income)
2 in developing countries (low to middle income)
1 in both developed and developing countries
10. Literature search results (cont.) All 11 papers evaluated population-wide salt reduction programs (some are hypothetical scenarios)
Either through cooperation between government and the food industry for stepwise deceases in salt content of processed foods, plus labeling, or
Legislation to decrease salt content in processed foods and appropriate labeling.
11. Study design and methods used in the literature Studies in developed countries
Markov modeling
Dynamic simulation model
Contingent valuation (willingness-to-pay)
Studies in developing countries
WHO Comparative Risk Assessment
WHO-Choice methodology
12. Major strengths of the literature Advanced Markov and dynamic simulation modeling techniques were employed.
Studies used the best data available , such as large national surveys, and information from the literature.
13. Major weaknesses of the literature Studies analyzed either medical cost saving from the intervention, or intervention costs only. Thus, they may not be comprehensive cost-effectiveness studies.
14. Main findings: interventions in developed countries Five studies in the US: Bibbins-Domingo (2010), Smith-Spangler (2010), Palar (2009), Dall (2009.1), and Dall (2009.2)
All used Markov and simulation modeling
Analyzed effects on US adults
Health outcomes were coronary heart disease, stroke, myocardial infarction, hypertension, quality-adjusted-life-years, and mortality.
15. Main findings: developed countries (cont) Findings from Bibbins-Domingo (2010):
The reduction in salt intake of 3g per day would save $10 to $24 billion in health care costs annually.
The intervention would be cost saving with even a modest reduction of 1g per day, and more cost-effective than using medications to lower blood pressure.
16. Main findings: developed countries (cont) Findings from Smith-Spangler (2010):
Government collaboration with the food industry to voluntarily cut sodium in processed foods is more cost-effective than a sodium tax.
However, both approaches would improve health and save billions of dollars ($32 billions in medical cost saving from government collaboration, and $22 billion from a sodium tax over a lifetime.)
17. Main findings: developed countries (cont) Findings from Palar (2009):
Reducing average population sodium intake to 2300 mg/day, the recommended maximum for adults, may save $18 billion health care costs.
Large benefits to society may result from efforts to lower sodium consumption on a population level by modest amounts over time.
18. Main findings: developed countries (cont) Findings from Dall (2009.1) and (2009.2):
Long-term sodium intake reductions of 400 mg/d in those with uncontrolled hypertension would save $2.3 billion annually.
It would also potentially increase productivity by $2.5 billion annually.
19. Main findings: developed countries (cont) Other three studies (Canada, Denmark, and Norway)
Canada: lowering sodium intake results in health care cost saving of $430 million per year; physician visits and laboratory costs decreased by 6.5%
Denmark: willingness-to-pay from the public for sodium reduction was $468 million, higher than the annual program cost of $148 million. The program was warranted from an economic point of view.
In Norway, the intervention lead to health care cost saving $118 million from fewer stroke and heart attacks.
20. Main findings: interventions in developing countries Two studies: Argentina (Rubinstein, 2009), and 23 low to middle income countries (Asaria, 2007)
Both used methods developed in WHO: Comparative Risk Assessment and Generalized cost-effectiveness analysis.
21. Main findings: developing countries (cont) Findings from Rubinstein (2009):
The reduction in salt intake is the most cost-effective strategy (only $151 per DALY) in reducing cardiovascular disease compared with other strategies such as mass media campaign ($547), drug therapy ($3,599), and tobacco cessation programs ($33,563).
..
22. Main findings: developing countries (cont) Findings from Asaria (2007):
The cost of salt reduction program was less than $0.40 per person per year. Thus, it could be implemented without great cost or structural change to the health system, and it could make a major contribution in reducing death rate from chronic diseases.
23. Main findings: interventions in developed and developing countries Murray (2003), is the only study that covers both developed and developing countries (Southeast Asia, Latin America, and Europe), used the method developed through WHO-Choice project.
The method allows interventions to be put into broad categories, such as very cost-effective, cost-effective, and cost ineffective, revealing the extent to which strategies to reduce risks to health differ across different settings.
24. Main findings: developed and developing countries Murray (2003)
In all regions, salt reduction through voluntary agreements with industry, as well as population-wide reduction in salt intake legislation are very cost-effective for cardiovascular disease prevention.
25. Conclusions All the studies provided the cost-effectiveness evidence that is in favor of population-based salt reduction interventions.
Studies in US and Canada used medical cost saving, while studies in other regions used implementation costs for the cost-effectiveness evaluations.
Low costs by total program and per capita costs.
. .
26. What next
Cost-effectiveness is one of the key inputs for policy makers to make informed resource-allocation decisions.
How the cost-effectiveness evidence informs policy making need to be explored.
The number of cost-effectiveness analyses is small.
Empirical research on community interventions and economic evaluations in the US.