Download
1 / 73
950 likes | 2.4k Views
Wound Dressing & Artificial Skin. Introduction. Our skin is a major organ of the body that acts as a barrier to pathogens and trauma . Skin defects caused by burns, venous and diabetic ulcers, or acute injury occasionally induce life-threatening situations. . Introduction.

E N D
Introduction • Our skin is a major organ of the body that acts as a barrier to pathogens and trauma. • Skin defects caused by burns, venous and diabetic ulcers, or acute injury occasionally induce life-threatening situations.
Introduction • Many burned people die, their body couldn’t produce new skin • Skin is largest organs in the body • Skin is important to protect body from infection and harmful bacteria • Skin keep vital fluid in
Functions of Skin? • Skin is the largest organ in the human body • Helps preserve fluid balance • Controls body temperature • Helps prevent and fight diseases
Wounds • What are wounds ? • Break in skin or mucous membranes • Any breach in the surface of the body or any tissue disruption produced by the application of energy • Usually physical injury • Abrasion injury • Contusion, crush injury • Incision, laceration
The Anatomy of Human Skin • Epidermis (5 layers) Keratinocytes provide protective properties. Melanocytes provide pigmentation. Langerhans’ cells help immune system. Merkel cells provide sensory receptors. • Dermis (2 layers) Collagen, glycoaminoglycans, elastine, ect. Fibroblasts are principal cellular constituent. Vascular structures, nerves, skin appendages. • Hypodermis (fatty layer) Adipose tissue plus connective tissue. Anchors skin to underlying tissues. Shook absorber and insulator.
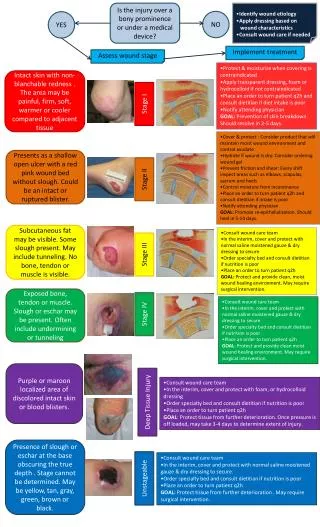
Wound Classification • Superficial • Deep (blood vessels, nerves, muscle, tendons, ligaments, bones) • Open Wound • Superficial or deep break in skin (abrasion, puncture, laceration)
Wound Classification • Closed: blunt force; twisting, turning, straining, bone fracture, visceral organ tear • Acute: trauma sharp object or blow • Surgical incision, gun shot, venipuncture • Chronic: pressure ulcers • Causality • Intentional: surgical incision • Unintentional: traumatic • Knife • Burn
Wound Healing • Primary Intention • skin edges are approximated (closed) as in a surgical wound • Inflammation subsides within 24 hours (redness, warmth, edema) • Resurfaces within 4 to 7 days • Secondary Intention: tissue loss • Burn, pressure ulcer, severe laceration • Wound left open • Scar tissue forms
Wound Healing Phases • Inflammatory Response • Serum and RBC’s form fibrin network • Increases blood flow with scab forming in 3 to 5 days • Proliferative Phase: 3-24 days • Granulation tissue fills wound • Resurfacing by epithelialization • Remodeling: more than 1 year • collagen scar reorganizes and increases in strength • Fewer melanocytes (pigment), lighter color
Some Factors Influencing Wound Healing • Age • Nutrition: protein and Vitamin C intake • Obesity decreased blood flow and increased risk for infection • Tissue contamination: pathogens compete with cells for oxygen and nutrition • Hemorrhage • Infection: purulent discharge • Dehiscence: skin and tissue separate • Evisceration: protrusion of visceral organs • Fistula: abnormal passage through two organs or to outside of body
Wound Healing • As wound heals: • Fluid and cells drain from damaged tissue • Exudate may be: • Clear • Bloody • Pus-containing • Proper wound healing: • Cleanliness and care of lesion • Proper circulation • Good general health and nutrition
Wound Healing • Vascular Response • Blood coagulation • Inflammation • Formation of new tissue • Epithelialisation • Contraction & Remodeling
Phases of healing • Inflammatory • Bleeding/clotting • Migration of WBCs • Cell swelling • Reparative • Laying down of collagen + migration of epith. cells • New capillary loops • Proliferation of fibroblastsstrands of collagen • Consolodative • reorientation +contraction of collagen • collagen synthesisdegradation • vascularity
Burn Injuries • Statistics • Annually, there are approximately 1.25 million people in the US who sustain burn injuries • Of these, 5,500 do not survive and 51,000 require hospitalization • Persons whose burn injuries require hospitalization have about a 50% chance of sustaining temporary or permanent disability • The most common part of the body involved in burn injury is an upper extremity, followed by the head and neck
Burn Classification - Cause • The primary cause of burn injury is exposure to temperature extremes • Heat injuries are more frequent than cold injuries • Cold injuries almost exclusively result from frostbite • Electrical and chemical injuries constitute 5-10% of burn injuries and are largely the result of occupational accidents
Effects • Burn injury causes destruction of tissue, usually the skin, from exposure to thermal extremes (either hot or cold), electricity, chemicals, and/or radiation • The mucosa of the upper GI system (mouth, esophagus, stomach) can be burned with ingestion of chemicals • The respiratory system can be damaged if hot gases, smoke, or toxic chemical fumes are inhaled • Fat, muscle, bone, and peripheral nerves can be affected in electrical injuries or prolonged thermal or chemical exposure • Skin damage can result in altered ability to sense pain, touch, and temperature
Old terminology 1st degree: only the epidermis 2nd degree: epidermis and dermis, excluding all the dermal appendages 3rd degree: epidermis and all of the dermis 4th degree: epidermis, dermis, and subcutaneous tissues (fat, muscle, bone, and peripheral nerves) New terminology Superficial: only the epidermis Superficial partial thickness: epidermis and dermis, excluding all the dermal appendages Deep partial thickness: epidermis and most of the dermis Full thickness: epidermis and all of the dermis Burn Classification - Depth
PRIMARY WOUND DRESSINGSPrimary wound dressing is applied directlyto wounds to protect from contamination,absorb exudates and facilitate healing.They are in the form of:•Self adhesives and do not need a secondary dressing.•An interface layer between the wound andthe secondary dressing.
CHARACTERSTICS OF IDEALWOUND DRESSING • Maintain humidity • Remove excess exudates • Allow gaseous exchange • Provide thermal insulation • Impermeable to bacteria • Allow removal without causing trauma • Non toxic and non allergenic • Cost effective • Availability
Wound Dressing Selection: Types and Usage • Gauze Dressings • Transparent Films • Foams • Hydrocolloids • Alginates • Composites
Gauze dressings • Woven or non-woven materials • Wide variety of shapes and sizes. • Use on: infected wounds, wounds which require packing, wounds that are draining, wounds requiring very frequent dressing changes. • Pros: readily available; cheaper than other dressing types; can be used on virtually any type of wound. • Cons: must be changed frequently, which may add to overall cost; may adhere to the wound bed; must often be combined with another dressing type; often not effective for moist wound healing.
Transparent film dressings • Allow oxygen to penetrate through the dressing to the wound, while simultaneously allowing moisture vapor to be released. • Composed of a polyurethane material. • Use on: partial-thickness wounds, donor sites, minor burns, stage I and II pressure ulcers. • Pros: conforms to the wound well, can stay in place for up to one week; aids in autolytic debridement; prevents friction against the wound bed; does not need to be removed to visualize the wound; keeps the wound bed dry and prevents bacterial contamination of the wound. • Cons: may stick to some wounds, not suitable for heavily draining wounds, may promote periwound maceration due to its occlusive nature.
Foams • Less apt to stick to delicate wound beds, are non-occlusive and are composed of a film coated gel or a polyurethane material which is hydrophilic in nature. • Use on: pressure ulcers, minor burns, skin grafts, diabetic ulcers, donor sites, venous ulcers. • Pros: comfortable, won’t adhere to the wound bed, and highly absorbent; allow for less frequent dressing changes, depending on the amount of wound exudate; come in many shapes and sizes. • Cons: may require a secondary dressing to hold the foam in place; if not changed often enough may promote periwound maceration; cannot be used on wounds with eschar or wounds that are not draining.
POLYUNETHANE FOAM DRESSING • Varying types and with different performance features and indications. • Available in both non adhesive and adhesive. • Allows absorption of exudates. • Uses: Traumatic wounds, Leg ulcers, Minor Burns, • Donor sites. • Examples: • •Lyofoam – allows passage of fluid • •Allevyn – has low-adhering wound contact with moderate exudates • •Tielle – allows vapour escape with low exudates.
Hydrocolloid dressings • Very absorbent and contain colloidal particles such as methylcellulose, gelatin or pectin that swell into a gel-like mass when they come in contact with exudate. • Strong adhesive backing. • Use on: burns, pressure ulcers, venous ulcers. • Pros: encourage autolytic debridement; provide insulation to the wound bed; waterproof and impermeable to bacteria, urine or stool; provide moderate absorption of exudate. • Cons: leave a residue present in the wound bed which may be mistaken for infection; may roll over certain body areas that are prone to friction; cannot be used in the presence of infection.
HYDRO GEL DRESSINGS • Consist of insoluble polymers with hydrophilic sites, which interact with aqueous solutions, absorb and retain water. • Key Features: • Removes slough and necrotic tissue by rehydrating dead tissue and enabling autolytic debridement. • Carries metronidazol to treat fungal and other malodorous wounds. • Uses: Sinuses, Infected wounds, Sloughs and necrotic wounds. • Examples: • Intrasite gel, Neugel, Granugel.
Alginates • Contain salts derived from certain species of brown seaweed. • Woven or nonwoven • Form a hydrophilic gel when they come in contact with exudate from the wound. • Use on: venous ulcers, wounds with tunneling, wounds with heavy exudate. • Pros: highly absorbent; may be used on wounds that have infection present; are non-adherent; encourage autolytic debridement. • Cons: always require a secondary dressing, may cause desiccation of the wound bed, as well as drying exposed tendon, capsule or bone (should not be used in these cases).
ALGINATE DRESSINGS • Consist, principally of calcium salts of alginic acid, a polysaccharide derived from seaweed. • Key Features: • The calcium alginate in contact with the wound exudates forms a gel on the wound surface that is believed to facilitate healing. • The chemical and physical properties differ in the varieties of alginate on available. • Plain or impregnated with silver. Examples: • Saesorb, Kaltogel, Kaltostat, Sorbsan, Tegagen, Acquacel.
Composites • May be used as the primary dressing or as a secondary dressing. • Made from any combination of dressing types, but are merely a combination of a moisture retentive dressing and a gauze dressing. • Use on: a wide variety of wounds, depending on the dressing. • Pros: widely available; simple for clinicians to use. • Cons: may be more expensive and difficult to store; less choice/flexibility in indications for use.
The best material for wound closure is the patient’s own skin; however autografting has several disadvantages: • The donor site is a new wound. • Scarring and pigmentation changes occur. • Dermis is not replaced. • Donor site is a potential site for infection. • Donor site is not unlimited. • Extensive burns makes it impossible.
Xenografts • Xenografts, particularly porcine skin grafts, are • commercially available and are an effective means of short-term wound closure . • A Xenograft is normally removed on the third or • fourth day of use before extensive adhesion onto the wound bed sets in, thereby necessitating its traumatic excision prior to drying and sloughing off.
Cadaver Skin: Allograft as a Temporary Skin Substitute • The annual national requirement for cadaver skin is estimated to be only 3000 m2. • Yet only 14% to 19% of human skin needed is being recovered.