Download
1 / 22
220 likes | 313 Views
University of Texas ICU Collaborative. Lessons Learned…. UT ICU Collaborative Proposal. University of Texas Fellowship for Quality and Patient Safety Proposed Project Description Sherry Martin, VP, Quality Management, M.D. Anderson Cancer Center

E N D
University of Texas ICU Collaborative Lessons Learned…
UT ICU Collaborative Proposal University of Texas Fellowship for Quality and Patient Safety Proposed Project Description Sherry Martin, VP, Quality Management, M.D. Anderson Cancer Center Intensive Care Units are inherently costly and unsafe. There are nearly 5 million ICU admissions each year in the U.S.; accounting for about 30% of hospital costs ($180 Billion/yr)(Birkmeyer, 2000). Nearly every patient admitted to an ICU suffers an adverse event (Pronovost, 2002). Despite more than 50 years of learning and experience in critical care, ICU mortality rates average 10-20% in most hospitals. Overall, approximately 500,000 patients die in U.S. ICU’s each year (Zimmerman,1998). Tremendous attention and resources have been focused on understanding the culture of the ICU with the intention of enhancing patient safety and outcomes, reducing attributable morbidity and mortality, and improving the utilization of scarce resources. This impetus for change in the ICU comes from the medical profession (Society of Critical Care Medicine), regulatory agencies (JCAHO) and healthcare consumers (Leapfrog Group). Many ICU’s are in the process of identifying and implementing best practices in order to comply with these requirements. These focused efforts have led to measurable improvements in outcomes. For example, a 66% reduction in adverse drug events in ICU’s with clinical pharmacist participation in daily ICU multidisciplinary rounds and a 50% reduction of LOS using ventilator pneumonia prevention methods (Pronovost, 2002).
UT ICU Collaborative Proposal University of Texas Fellowship for Quality and Patient Safety Proposed Project Description Sherry Martin, VP, Quality Management, M.D. Anderson Cancer Center Intensive Care Units are inherently costly and unsafe. There are nearly 5 million ICU admissions each year in the U.S.; accounting for about 30% of hospital costs ($180 Billion/yr)(Birkmeyer, 2000). Nearly every patient admitted to an ICU suffers an adverse event (Pronovost, 2002). Despite more than 50 years of learning and experience in critical care, ICU mortality rates average 10-20% in most hospitals. Overall, approximately 500,000 patients die in U.S. ICU’s each year (Zimmerman,1998). Tremendous attention and resources have been focused on understanding the culture of the ICU with the intention of enhancing patient safety and outcomes, reducing attributable morbidity and mortality, and improving the utilization of scarce resources. This impetus for change in the ICU comes from the medical profession (Society of Critical Care Medicine), regulatory agencies (JCAHO) and healthcare consumers (Leapfrog Group). Many ICU’s are in the process of identifying and implementing best practices in order to comply with these requirements. These focused efforts have led to measurable improvements in outcomes. For example, a 66% reduction in adverse drug events in ICU’s with clinical pharmacist participation in daily ICU multidisciplinary rounds and a 50% reduction of LOS using ventilator pneumonia prevention methods (Pronovost, 2002). Project Purpose: To create a multidisciplinary program focused on ICU quality initiatives that will enhance patient safety, utilization of resources, and healthcare provider satisfaction and to facilitate collaboration among participating institutions to improve practices through shared knowledge.
ICU Collaborative • “Best Practice Fever” • Shared Knowledge and Experiences • Data-driven Practice • ICU Registry
ICU Collaborative Survey University of Texas System Health Components Survey Intensive Care Unit Quality Improvement Strategies Please complete the following survey about your critical care unit(s). Aggregate results will be available to participants following the Steering Committee Conference. Please submit any other information or explanations on a separate sheet. All submitted information will remain confidential. Institution: □ The University of Texas Southwestern Medical Center , Dallas □ The University of Texas Medical Branch, Galveston □ The University of Texas Health Science Center, Houston □ The University of Texas Health Science Center, San Antonio □ The University of Texas Health Center, Tyler □ The University of Texas M.D. Anderson Cancer Center What types of critical care units are present in your institution? (check all that apply): □ Medical ICU □ Surgical ICU □ Medical/Surgical ICU □ Cardiothoracic Surgical ICU □ Transplant ICU □ Coronary Care Unit □ Pediatric ICU □ Neonatal ICU □ Burn ICU □ Trauma ICU □ Intermediate Care Unit □ Telemetry Unit □ Other: ____________ □ Other: ____________ Do you utilize a multidisciplinary team approach to critical care? Yes / No
ICU Collaborative Survey University of Texas System Health Components Survey Intensive Care Unit Quality Improvement Strategies Please complete the following survey about your critical care unit(s). Aggregate results will be available to participants following the Steering Committee Conference. Please submit any other information or explanations on a separate sheet. All submitted information will remain confidential. Institution: □ The University of Texas Southwestern Medical Center , Dallas □ The University of Texas Medical Branch, Galveston □ The University of Texas Health Science Center, Houston □ The University of Texas Health Science Center, San Antonio □ The University of Texas Health Center, Tyler □ The University of Texas M.D. Anderson Cancer Center What types of critical care units are present in your institution? (check all that apply): □ Medical ICU □ Surgical ICU □ Medical/Surgical ICU □ Cardiothoracic Surgical ICU □ Transplant ICU □ Coronary Care Unit □ Pediatric ICU □ Neonatal ICU □ Burn ICU □ Trauma ICU □ Intermediate Care Unit □ Telemetry Unit □ Other: ____________ □ Other: ____________ Do you utilize a multidisciplinary team approach to critical care? Yes / No Who are the ICU Multidisciplinary Team Members (check all that apply): □ Certified Intensivist □ Non ICU-certified Staff Physician □ Critical Care Fellow □ Resident □ Medical Student □ Nursing Student □ Pharmacy Student □ Physician Assistant □ Advanced Practice Nurse □ Pharmacist □ Respiratory Therapist □ Physical/Occupational Therapist □ Nutrition Specialist □ Clinical Ethicist □ Chaplain □ Other ______________
ICU Collaborative Survey University of Texas System Health Components Survey Intensive Care Unit Quality Improvement Strategies Please complete the following survey about your critical care unit(s). Aggregate results will be available to participants following the Steering Committee Conference. Please submit any other information or explanations on a separate sheet. All submitted information will remain confidential. Institution: □ The University of Texas Southwestern Medical Center , Dallas □ The University of Texas Medical Branch, Galveston □ The University of Texas Health Science Center, Houston □ The University of Texas Health Science Center, San Antonio □ The University of Texas Health Center, Tyler □ The University of Texas M.D. Anderson Cancer Center What types of critical care units are present in your institution? (check all that apply): □ Medical ICU □ Surgical ICU □ Medical/Surgical ICU □ Cardiothoracic Surgical ICU □ Transplant ICU □ Coronary Care Unit □ Pediatric ICU □ Neonatal ICU □ Burn ICU □ Trauma ICU □ Intermediate Care Unit □ Telemetry Unit □ Other: ____________ □ Other: ____________ Do you utilize a multidisciplinary team approach to critical care? Yes / No Which of the following ICU protocols or pathways are in use? (check all that apply): □ ICU Admission Orders □ Electrolyte Replacement □ Analgesia □ Sedation □ Delirium □ Neuromuscular Blockade □ Ventilator Weaning □ Non-Invasive Ventilation □ Pulmonary Toilet □ Vasoactive Medication □ Heparin Infusion □ Glucose control/Insulin sliding scale □ Glucose control/Insulin infusion □ DVT prophylaxis □ GI Stress Ulcer prophylaxis □ Enteral nutrition □ Parenteral Nutrition PPN/TPN □ Blood Product Transfusion □ Empiric Antimicrobial Therapy □ Bowel Management □ Renal Replacement Therapy □ Restraints □ End-of-Life/Palliative Care □ Intracranial Pressure Management □ “Bundles” □ Other: __________________
ICU Collaborative Survey University of Texas System Health Components Survey Intensive Care Unit Quality Improvement Strategies Please complete the following survey about your critical care unit(s). Aggregate results will be available to participants following the Steering Committee Conference. Please submit any other information or explanations on a separate sheet. All submitted information will remain confidential. Institution: □ The University of Texas Southwestern Medical Center , Dallas □ The University of Texas Medical Branch, Galveston □ The University of Texas Health Science Center, Houston □ The University of Texas Health Science Center, San Antonio □ The University of Texas Health Center, Tyler □ The University of Texas M.D. Anderson Cancer Center What types of critical care units are present in your institution? (check all that apply): □ Medical ICU □ Surgical ICU □ Medical/Surgical ICU □ Cardiothoracic Surgical ICU □ Transplant ICU □ Coronary Care Unit □ Pediatric ICU □ Neonatal ICU □ Burn ICU □ Trauma ICU □ Intermediate Care Unit □ Telemetry Unit □ Other: ____________ □ Other: ____________ Do you utilize a multidisciplinary team approach to critical care? Yes / No What has been your greatest ICU Quality Improvement success? What has been your greatest ICU Quality Improvement challenge? What should be the top priority for the University of Texas System Health Components Intensive Care Unit Quality Improvement Project?
ICU Collaborative • “Make it easier to ‘Do the Right Thing’” • Terry Clemmer, MD • “Rapid Cycle Improvement in ICU” • “War Wounds” • Brainstorming
Barriers • “Changing a tire on a moving vehicle” • Different Institutions, Different Patients • “OK, but not in my patients” • Quality Improvement Tools • Facilitator • “Data Gap”
Glucose Management • Protocol • Mass Customization • Outcomes • “Tight Glucose Management” • Hypoglycemia
Grp1 (Jun - Aug 04) 98 events 0.87% event rate 46 unique patients Average age - 59 yrs 11 surgical patients 35 medical patients Grp2 (Feb - May 05) 116 events 0.55% event rate 59 unique patients Average age - 51 yrs 16 surgical patients 43 medical patients Demographics
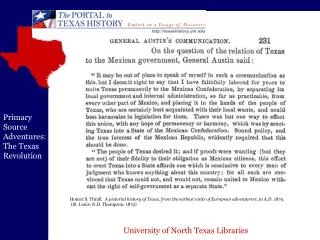
Comparison of Patients with Hypoglycemic Events 'On or Off' Insulin Protocols
Request for a University of Texas System Grant To Support System-wide Collaborative Efforts Introduction: The University of Texas System ICU Collaborative was formed as a Chancellor’s Health Fellow project in 2004 and has been operational since that date. The purpose of the ICU Collaborative is to develop the infrastructure and processes necessary to establish system-wide, enduring collaborations within the UT System healthcare components focused on the improvement of effective, efficient, and safe patient care. This collaboration provides a pathway for studying healthcare delivery across a large number of intensive care unit beds, which may be the largest collaborative source of ICU beds within the nation. The diversity of patient populations within these ICUs enables comparison of methods and transfer of this learning to organizations cross the nation. Participants in the Collaborative have been introduced to basic quality improvement methodology. During the first two years, intensive care units in various healthcare components and affiliated hospitals shared protocols to manage glucose and control ventilator-associated pneumonia. They agreed upon targets to achieve, shared data and presented their results in group meetings. Results of these meetings led to changes in their own protocols and subsequently to modifications of protocols to improve glucose management and ventilator associated pneumonia control..
Request for a University of Texas System Grant To Support System-wide Collaborative Efforts Introduction: The University of Texas System ICU Collaborative was formed as a Chancellor’s Health Fellow project in 2004 and has been operational since that date. The purpose of the ICU Collaborative is to develop the infrastructure and processes necessary to establish system-wide, enduring collaborations within the UT System healthcare components focused on the improvement of effective, efficient, and safe patient care. This collaboration provides a pathway for studying healthcare delivery across a large number of intensive care unit beds, which may be the largest collaborative source of ICU beds within the nation. The diversity of patient populations within these ICUs enables comparison of methods and transfer of this learning to organizations cross the nation. Participants in the Collaborative have been introduced to basic quality improvement methodology. During the first two years, intensive care units in various healthcare components and affiliated hospitals shared protocols to manage glucose and control ventilator-associated pneumonia. They agreed upon targets to achieve, shared data and presented their results in group meetings. Results of these meetings led to changes in their own protocols and subsequently to modifications of protocols to improve glucose management and ventilator associated pneumonia control.. • CGMS Research Protocol • The complete CGMS Research Protocol as presented to the Institutional Review • Boards of the participating Institutions is found in Attachment A • The expected outcomes of the CGMS protocol include: • The determination of the accuracy of the continuous glucose monitoring • device as compared to the current glucose measures, publications for the • participating faculty, • A potential decrease in number of invasive “sticks” or phlebotomy that a • patient may encounter in the ICU when on an insulin drip • Potential decrease in nursing workload if continuous glucose monitor is as • accurate as current standard of glucose monitoring with hourly blood • draws.
Request for a University of Texas System Grant To Support System-wide Collaborative Efforts Introduction: The University of Texas System ICU Collaborative was formed as a Chancellor’s Health Fellow project in 2004 and has been operational since that date. The purpose of the ICU Collaborative is to develop the infrastructure and processes necessary to establish system-wide, enduring collaborations within the UT System healthcare components focused on the improvement of effective, efficient, and safe patient care. This collaboration provides a pathway for studying healthcare delivery across a large number of intensive care unit beds, which may be the largest collaborative source of ICU beds within the nation. The diversity of patient populations within these ICUs enables comparison of methods and transfer of this learning to organizations cross the nation. Participants in the Collaborative have been introduced to basic quality improvement methodology. During the first two years, intensive care units in various healthcare components and affiliated hospitals shared protocols to manage glucose and control ventilator-associated pneumonia. They agreed upon targets to achieve, shared data and presented their results in group meetings. Results of these meetings led to changes in their own protocols and subsequently to modifications of protocols to improve glucose management and ventilator associated pneumonia control.. Information Systems Gap Analysis If funded, the UT System ICU Collaborative proposes to retain Sentigy, an information systems consulting group that falls under the State of Texas Historically Underutilized Business (HUB) classification, to perform the gap analysis. Sentigy has performed work at several of the UT System components and thus is familiar with the information systems. They will be requested to conduct an evaluation of the ability of the information systems at the participating organizations to collect and transfer data that will be required to participate effectively in the ICU CGMS research protocol. This evaluation should include a gap analysis for organizations currently unable to manage data effectively and recommendations to achieve this goal. This will then address the first step necessary to achieve a a UT System-wide ICU Registry. The registry will be a powerful tool similar to tumor registries (such as the M. D. Anderson Tumor Registry) and trauma registries found in many centers or regions.
Request for a University of Texas System Grant To Support System-wide Collaborative Efforts Introduction: The University of Texas System ICU Collaborative was formed as a Chancellor’s Health Fellow project in 2004 and has been operational since that date. The purpose of the ICU Collaborative is to develop the infrastructure and processes necessary to establish system-wide, enduring collaborations within the UT System healthcare components focused on the improvement of effective, efficient, and safe patient care. This collaboration provides a pathway for studying healthcare delivery across a large number of intensive care unit beds, which may be the largest collaborative source of ICU beds within the nation. The diversity of patient populations within these ICUs enables comparison of methods and transfer of this learning to organizations cross the nation. Participants in the Collaborative have been introduced to basic quality improvement methodology. During the first two years, intensive care units in various healthcare components and affiliated hospitals shared protocols to manage glucose and control ventilator-associated pneumonia. They agreed upon targets to achieve, shared data and presented their results in group meetings. Results of these meetings led to changes in their own protocols and subsequently to modifications of protocols to improve glucose management and ventilator associated pneumonia control.. • Clinical Safety and Effectiveness (CS&E) Course • ICU teams participating in the CGMS research protocol will attend the M. D. Anderson CS&E course to develop skills and knowledge necessary to conduct improvement initiatives. Support is requested for two individuals, one physician (the protocol principal investigator) from each participating UT organization and one nurse from the affiliated hospital’s ICU. Each team will participate in the CS&E course to be held at M. D. Anderson in the fall of 2007. These teams will use the CGMS protocol as their course projects and the course will emphasize this protocol throughout the lectures.
ICU Collaborative • Healthcare Delivery Projects • Institutional Projects • UT System Projects • Clinical Research Projects • CGMS Project • eProtocol insulin • Indwelling Glucose Monitoring device
UT System Collaboratives • Join one! • Build one! • Support them!