Download
1 / 85
990 likes | 2.19k Views
Overview of Psoriasis. Adam O. Goldstein, MD, MPH Associate Professor UNC Department of Family Medicine Email: aog@med.unc.edu. Objectives. 1 . Differentiate psoriasis types 2. Form differential dx 3. Review tx guidelines 4. Review new products

E N D
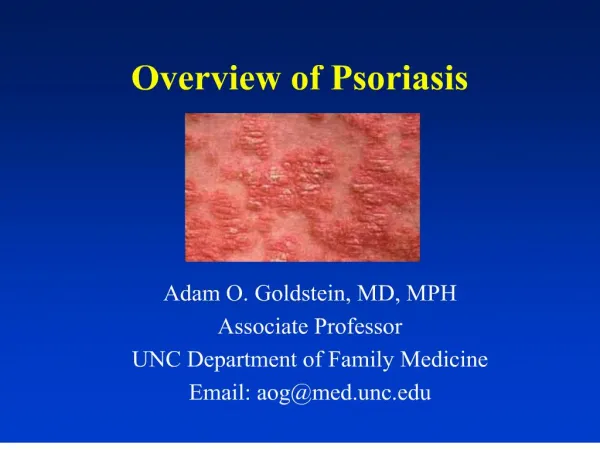
Overview of Psoriasis Adam O. Goldstein, MD, MPH Associate Professor UNC Department of Family Medicine Email: aog@med.unc.edu
Objectives 1. Differentiate psoriasis types 2. Form differential dx 3. Review tx guidelines 4. Review new products 5. Learn 2 additional patient education pearls
“I am silvery, scaly. Puddles of flakes form wherever I rest my flesh.... Lusty, though we are loathsome to love. Keen-sighted, though we hate to look upon ourselves. The name of the disease, spiritually speaking, is…. Humiliation
Psoriasis: Incidence • 2-3% U.S. (6.4 million) • 200,000 new cases/year • 300,000 have >20% BSA • Median age dx: 30 • Two peaks: 16-22, 57-60 • Costs: $2 billion/year • Mean per patient costs $3000 (Javitz, J Am Acad Dermatol, 2002)
Psoriasis: Quality of Life • 50% seek treatment • As debilitating as other chronic illnesses • > rates depression & alcohol abuse (Sharma, J Dermatol, 2001)
Case • Bob- 34 yo insurance executive • history of psoriasis for 8 years • scalp, elbows, knees and trunk • Got topical steroid (Psorcon E, 60 gms) from dermatologist 3 years ago • helped with itching • Wants a renewal and wonders if needs to see a dermatologist • You estimate 5-10% involvement of skin with plaque psoriasis
Case What is your treatment plan? Do you refer him to a dermatologist?
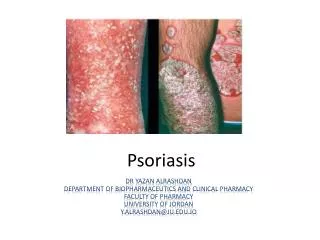
Psoriasis: Definition • Chronic, remitting and relapsing • Scaly and inflammatory • Genetically influenced
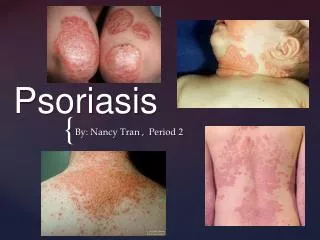
Psoriasis: • Morphology: Circumscribed, thickened, plaques with secondary erythema and thick, silvery scales
Psoriasis: Pathogenesis • Hyperproliferation of the epidermis • Normal skin cell matures in 28-30 days • Psoriatic skin cell matures in 3-6 days
Psoriasis: Types • Plaque-typeLocalized or Generalized • PustularLocalized or Generalized
Psoriasis • Arthritis associated (5-7%)
Psoriasis: Distribution (From Pardasan AG, et al. Am Fam Physician 2000)
Psoriasis: Distribution • Extensor
Psoriasis: Distribution • Extensor
Psoriasis: Distribution • Nails
Psoriasis: Distribution • Genitalia
Psoriasis: Distribution • Hands & feet
Psoriasis: Distribution • Pustular
Psoriasis: Distribution • Intertriginous/inverse- armpits, groin, under breasts(less thick “silvery”scale)
Psoriasis: Distribution • Guttate-small red dots (Gutta = drops) • Appears suddenly after a strep, URI, other infection, stress, medications
Psoriasis: Guttate • Appears after strep, URI, stress, medica-tions
Psoriasis: Distribution • Erythrodermic • Widespread erythema, itching, pain, edema
Psoriasis: Distribution • Sites of trauma (Koebner’s phenomenon)
Psoriasis: Diagnosis • Early on, may look like other diseases • Bx may be necessary
Psoriasis: Differential Diagnosis • Drug eruption
Psoriasis: Differential Diagnosis • secondary syphilis
Psoriasis: Differential Diagnosis • Seborrhea: Finer scale, central facial, scalp, central chest; Greasier; Sebopsoriasis
Psoriasis: Differential Diagnosis • dermatophyte infections (Tinea) • KOH negative • scale not as thick or silvery
Psoriasis: Differential Dx • intertriginous: diaper dermatitis/candidiasis • satellite pustules, beefy red, maceration; KOH positive for yeast in candidiasis; may coexist
Psoriasis: Differential Diagnosis • Eczema • Neuro-dermatitis/ lichen simplex chronicus
Psoriasis: Differential Dx • lichen planus
Psoriasis: Differential Diagnosis • lupus erythematosus
Psoriasis: Differential Diagnosis • pityriasis rosea
Psoriasis: Differential Diagnosis • Cutaneous T-cell lymphoma
Psoriasis: Principals of Treatment • Individualize treatment based on: • self-image, symptoms, interference with social interactions, expectations & scientific evidence • Patient education: Control, not cure • Pearl: • Combine products for better long-term control and fewer SE’s (Rees, J Am Acad Dermatol, 2003 )
Psoriasis: Treatment • Flares • skin injury (including dryness, scratching) • sunburn • infections (strep, HIV) • psychological stress • medications
Psoriasis: Treatment • Medications linked to psoriatic flares: • Lithium • Beta blockers • ACE inhibitors • Antimalarials • Indomethacin
PsoriasisPearl • Avoid systemic corticosteroids
Psoriasis: Treatment • <5% sunlight + topical tx • 5-20% sunlight + topical tx +/- systemic • >20% systemic tx +/- light therapy
Psoriasis: Treatment • Sunlight
Evidence-based medicine • No good evidence that non-drug tx’s work • Topical tx’s effective in short-term (few comparative RCT’s) • RCT’s show UVB and PUVA effective short/long term (long term risk PUVA-SCCa) • Cyclosporin clears short term but toxic (BMJ, Clinical Evidence 2001)
Psoriasis: < 20% BSATopical Therapies 1. Emollients 2. Keratolytic agents 3. Topical steroids 4. Calcipotriene 5. Tazarotene gel 6. Topical calcineurin inhibitors 7. Anthralin 8. Coal tar ( BMJ 2001)
1. Emollient cleansers and lotions/cream • Mild cleansers • Moisturizers
2. Keratolytic Agents • WHEN THE SCALE IS REALLY THICK Scalp: P & S liquid Body: 2-10% salicylic acid qd- bid
3. Topical Corticosteroids • Never treated- • start medium potency • follow up in 2 weeks • Previously treated • start high potency • 2-4 weeks, then taper • Always use lower potencies on face and intertriginous areas
3. Topical Corticosteroids • Creams most body parts • Lotions/mousse hairy areas • Ultrapotent/potent BID 2-3 weeks to thick lesions • Taper to weekend use only or: • Taper to Class III for maintenance to avoid atrophy/striae • Educate on: • “tolerance”, signs of atrophy, tapering & relapse • If topical steroids insufficient: • Steroids + occlusion (plastic wrap QHS- if no atrophy) • Steroids + calcipotriene cream/ointment or tazarotene gel • Coal tar products and/or Anthralin (Tristani-Firouzi, Cutis, 1998)
Intralesional injections • Isolated recalcitrant lesions TAC 3-10mg/cc in NS to plaques < 3 cm
4. Calcipotriene 0.005% (cream, ointment, solution) • Calcipotriene (Dovonex) • simulates differentiation • inhibits proliferation • > effective as steroids, tar, anthralin • > irritation than steroids • Use cautiously if renal or calcium-related conditions, especially (< 60 gm/week) • Use > 4 wks to determine effectiveness (BMJ 2001)