Download
1 / 62
630 likes | 865 Views
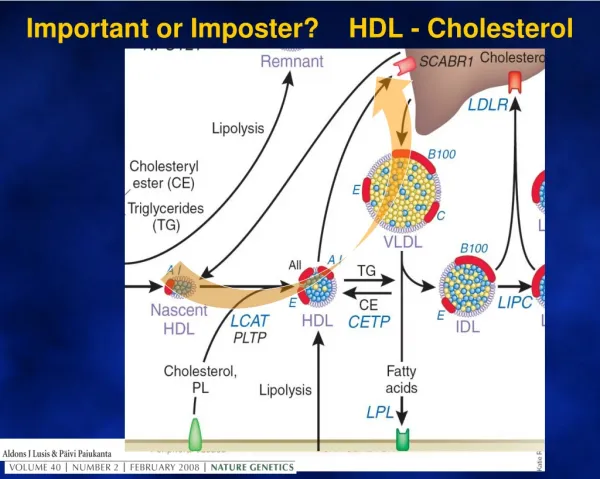
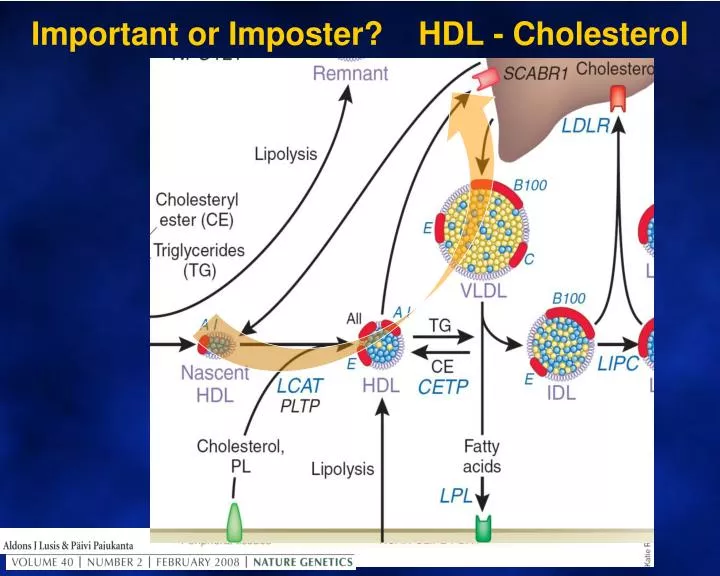
Important or Imposter? HDL - Cholesterol. The wider roles of HDL. Phospholipid. Glycosphingolipid. HDL and Reverse Cholesterol Transport. Membrane rafts are small (10–200 nm), heterogeneous cholesterol & sphingolipid -enriched domains. Cholesterol. Normal Cell Membrane. Lipid Raft.

E N D
Phospholipid Glycosphingolipid HDL and Reverse Cholesterol Transport Membrane rafts are small (10–200 nm), heterogeneous cholesterol & sphingolipid-enriched domains. Cholesterol Normal Cell Membrane Lipid Raft ABCA1 Diffusion ABCG1 SR-B1 Diffusion SR-B1 Lipid-poor apoAI Nascent, discoidal HDL CE Mature, spherical HDL LCAT
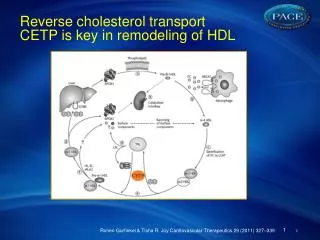
Pharmacologic Inhibition of CETP: A Novel HDL-raising Strategy Feces Bile A-I A-I FC CE CE FC LCAT FC FC CE ABCA1 SR-BI Macrophage Liver
Pharmacologic Inhibition of CETP: A Novel HDL-raising Strategy Feces Bile A-I A-I FC CE CE FC LCAT FC FC CE ABCA1 SR-BI Macrophage Liver CETP LDLR CE B TG VLDL/LDL
Liver receptor X (LXR) Promotes Reverse Cholesterol Transport: LXR Feces Bile ABCG1 LXR A-I A-I LXR BA LCAT FC FC FC LXR FC CE ABCA1 SR-BI ABCA1 Macrophage ABCA1 LXR FC
HDL Clinical Conditions CONDITION HDL level CVD risk Apo A1 deficiency absent severe Tangiers disease (ABC A1 defect) very low ? increased LCAT deficiency (& fish eye disease) very low ? uncertain Apo A1 Milano (dimer formation) very low ? reduced SRB1 deficiency (female infertility) very high ? unaltered CETP deficiency very high ? reduced
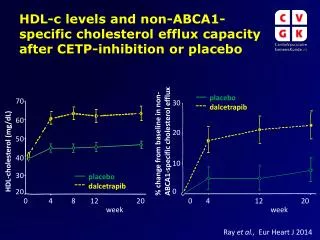
Beyond HDL-C: Laboratory assessment of reverse cholesterol efflux (by plasma)
HDL Therapy DRUG(S) Mechanism and HDL effect CVD effect Ezetimibe, fish oil Nil relevant? Neutral mild benefit BAS resins FXR Mild increase mild benefit StatinsHMGCoARI Mod. increase major benefit Fibrates PPAR alpha Mod. increase benefit in MS Niacin Reduced catabolism Increase ?benefit CETP Inhibitors CETPI Huge increase uncertain Novel (eg antiPCSK9) PCSK9 Mild increase uncertain
HDL Evidence: Epidemiology and trials STUDY or TRIAL HDL observation CVD effect Observational (eg Framingham) inverse relation protective Angiographic (Niacin, eg CLASS) large increase regression (CETP, eg ILLUSTRATE) large increase neutral RCT (Niacin, eg AIM-HIGH) large increase flawed neutral (Fibrate, eg VA-HIT) small increase protective (Fibrate in MS, eg FIELD) small increase protective (Torcetrapib, eg ILLUMINATE) very large increase detrimental (Dalcetrapib, eg DALOUTCOMES) large increase neutral
PotentialAntiatherogenic Actions of HDL VasodilatoryActivity Anti-inflammatory Activity Antithrombotic Activity HDL Antiapoptotic Activity Reverse Cholesterol Transport CellularCholesterolEfflux Anti-infectious Activity Antioxidative Activity EndothelialRepair Apo A-I Apo A-II Chapman MJ, et al. Curr Med ResOpin. 2004;20:1253-1268. Assmann G, et al. AnnuRev Med. 2003;53:321-341.
HDL composition is complex:Protein and phospholipid components
Plasma HDL Predicts Events in Population Studies * Men aged 50-70 3 2 CHD RISK 25 1 45 65 HDL-C (mg/dL) 85 0 100 220 160 LDL- cholesterol(mg/dL)
Structure of HDL Surface monolayer of phospholipids and free cholesterol apoA-I apoA-II Hydrophobic core of triglyceride and cholesteryl esters Note: LFA1 denotes Lipid Free Apo Lipoprotein A1 r HDL denotes Reconstituted HDL
Non-occlusive Silastic Peri-arterial Carotid Collar in Male NZ White Rabbits Collar Carotid artery
Treated Artery Post Two Infusions of LFA1 CD 18 B C A
Apo A1 Milano Infusions Lead to Significant Regression of Coronary Atherosclerosis(IVUS Study) . Nissen, S. E. et al. JAMA 2003;290:2292-2300
Mr A.M. Mr A.M. Is a 34 year old man of aboriginal descent who lives in rural NSW. His BP is 135 / 85. He was started on Rosuvastatin 20 mg because he has a very strong family history of premature cardiovascular disease (father, paternal aunt, 2 maternal uncles and older brother suffered onset of cardiovascular disease before age 45). Waistline is prominent and measures 98cms, but he is thin elsewhere. He had recurrent otitis media as a child and his dentition is poor. Follow-up lipids include TC=4.1, TG=2.9, HDL=0.5, LDL=2.3
Questions about Mr A.M. Is Mr A.M. eligible for Rosuvastatin according to Pharmaceutical Benefits Schedule Guidelines? Yes / No Mr A.M’s very low HDL-C is mainly due to A) Racial factors B) Intercurrent infection C) Central Obesity / Lifestyle D) Mendelian genetic factors E) Lack of exercise Which other racial groups have been documented to have relatively low HDL levels (2 correct). A) Kiwis B) Indians C) Finns D) Turkish E) Sub-Saharan Africans In rural NSW, the most feasible treatment to improve this man’s HDL-C is A) Fish oil B) An exercise programme C) Niacin D) Fibrate E) Antibiotic
Mr A.M. is a 34 year old man of aboriginal descent who lives in rural NSW. His BP is 135/85. He was started on Rosuvastatin 20 mg because he has a very strong family history of premature cardiovascular disease (father, paternal aunt, 2 maternal uncles and older brother suffered onset of cardiovascular disease before age 45). Waistline is prominent and measures 98cms, but he is thin elsewhere. He had recurrent otitis media as a child and his dentition is poor. Follow-up lipids include TC=4.1, TG=2.9, HDL=0.5, LDL=2.3 Mr A.M’s very low HDL-C is mainly due to A) Racial factors B) Intercurrent infection C) Central Obesity / Lifestyle D) Mendelian genetic factors E) Lack of exercise Is he eligible for Rosuvastatin according to Pharmaceutical Benefits Schedule Guidelines? Yes / No In rural NSW, the most feasible treatment to improve this man’s HDL-C is A) Fish oil B) An exercise programme C) Niacin D) Fibrate E) Antibiotic
Is Mr A.M. eligible for Rosuvastatin according to Pharmaceutical Benefits Schedule Guidelines? Yes / No
Is Mr A.M. eligible for Rosuvastatin according to Pharmaceutical Benefits Schedule Guidelines?Was “yes”, now “no”
Close the Gap scheme In Nov 2008 COAG agreed to $1.6 billion for CTG Benefit: Lower or nil payment for PBS medicines Eligible: Aboriginal/ Torres Strait Islander of any age who present with chronic disease or at risk of chronic disease AND would have significant setback from disease if they did not have Rx or unlikely to comply with out such assistance Register: at GP in the Indigenous Health Incentive under PIP or Indigenous Health services. Prescriber: Any in a practice participating in IHI under PIP or any in HIS or any specialist in any location if the patient is registered and the patient has been referred a doctor in IHI program. Script: CTG For more informationEmail: PBS-Indigenous@health.gov.au
Mr A.M’s very low HDL-C is mainly due to A) Racial factors B) Intercurrent infection C) Central Obesity / Lifestyle D) Mendelian genetic factors E) Lack of exercise
Mr A.M’s very low HDL-C is mainly due to..Reasons for a preference for “A”, “B” or “C”
Which other racial groups have been documented to have relatively low HDL levels ? A) Kiwis B) Indians C) Finns D) Turkish E) Sub-Saharan Africans
Which other racial groups have been documented to have relatively low HDL levels “B” supported by INTERHEART, but difficult to compare, eg “D”. ActaCardiol. 2007 Oct;62:453-9. Do Turkish adults really have lower serum levels of high-density lipoprotein cholesterol? Duran S, Memisogullari R, Coskun A, Yavuz O, Yuksel H. CONCLUSIONS: Our finding that the HDL-C level in this population was higher than the previously reported levels in Turkey indicates that HDL-C levels may not be as low as previously thought. We believe that lower HDL-C levels that were previously reported might be due to the difference between techniques of analysis, nutritional status, and percent of subjects who were fasting in the day of analysis or improper subject inclusion which did not reflect the Turkish population causing selection bias.
In rural NSW, the most feasible treatment to improve this man’s HDL-C is... A) Fish oil B) An exercise programme C) Niacin D) Fibrate E) Antibiotic
In rural NSW, the most feasible treatment to improve this man’s HDL-C is...The case for “D” Results Liver Circulation apo A-I Increased HDL Production … by controlling the expression of PPAR target genes apo A-II HDL ABCA1 ABCG1 Decreased VLDL Production VLDL apo C-III Apo A-V Increased VLDL Clearance TG FFA Decreased TG levels Acyl-CoA Synthase LPL Decreased small and dense LDL Particles LDL Acetyl CoA
More questions about Mr A.M. Mr A.M. has mild albuminuria. Would you add an antihypertensive, and if so, which of the following: A) Nil B) Diuretic C) CCB D) ACEI E) Moxonidine His lipids remain unaltered but his eGFR declines slightly to 55mls / min. Would you add A) Fenofibrate 48mg B) Fenofibrate 145 mg , but cease if creatinine increased by 25 umol/l C) Fenofibrate 145mg, but continue if creatinine increased by < 25umol/l) D) Fenofibrate 145 mg no matter what E) More rosuvastatin CVD risk can’t be calculated because low HDL makes TC:HDL too high for risk calculators. To further assess risk in this rural setting, would you A) Test ABI and hs-CRP locally B) Refer for regional exercise stress test C) Refer to a more distant regional centre for imaging (IMT) D) Refer to capital city for CT angio or coronary calcium score E) Not perform any of these investigations
Mr A.M. has mild albuminuria. Would you add an antihypertensive, and if so, which of the following: A) Nil B) Diuretic C) CCB D) ACEI E) Moxonidine
ease Mr A.M. has mild albuminuria. Would you add an antihypertensive, and if so, which of the following:The case for “D”
Mr A.M’s lipids remain unaltered but his eGFR declines slightly to 55mls / min. Would you add A) Fenofibrate 48mg B) Fenofibrate 145 mg , but cease if creatinine increased by 25 umol/l C) Fenofibrate 145mg, but continue if creatinine increased by < 25umol/l) D) Fenofibrate 145 mg no matter what E) More rosuvastatin
Mr A.M’s lipids remain unaltered but his eGFR declines slightly to 55mls / min. Would you add...The case for “C”
CVD risk can’t be calculated because low HDL makes TC:HDL too high for risk calculators. To further assess risk in this rural setting, would you... A) Test ABI and hs-CRP locally B) Refer for regional exercise stress test C) Refer to a more distant regional centre for imaging (IMT) D) Refer to capital city for CT angio or coronary calcium score E) Not perform any of these investigations
CVD risk can’t be calculated because low HDL makes TC:HDL too high for risk calculators. To further assess risk in this rural setting, would you...A survey of opinions
Mr S.K. This 37 year old man of Greek descent had routine tests in his 20’s that revealed a very low HDL-C (<0.2 mmol/l). He is a smoker who drinks 20 gms alcohol per week. He trains regularly as a body-builder. A cardiologist was sufficiently concerned to arrange angiography at age 33, which was normal. On examination there are no relevant physical findings and lipids are TC=2.2, TG=2.2, HDL-C =0.08, LDL-C=1.0mmol/l.
Questions concerning Mr S.K. Is his lipid disorder..... Primary / Secondary Are there any simple tests that would provide a diagnosis? Yes/No Which drugs can DRASTICALLY reduce HDL-C? (More than 1 possible) A) Diuretics B) Danazol C) Beta blockers C) Probocol E) Highly Active Antiretrovirals Your treatment would include A) Quit smoking advice only B) Niacin C) Statin D) Fibrate E) More alcohol
This 37 year old man of Greek descent had routine tests in his 20’s that revealed a very low HDL-C (<0.2 mmol/l). He is a smoker who drinks 20 gms alcohol per week. He trains regularly as a body-builder. A cardiologist was sufficiently concerned to arrange angiography at age 33, which was normal. On examination there are no relevant physical findings and lipids are TC=2.2, TG=2.2, HDL-C =0.08, LDL-C=1.0mmol/l. Is his lipid disorder..... Primary / Secondary Are there any simple tests that would provide a diagnosis? Yes/No Which drugs can DRASTICALLY reduce HDL-C? (More than 1 possible) A) Diuretics B) Danazole C) Beta blockers C) Anabolic steroids E) Highly Active Antiretrovirals Your treatment would include A) Quit smoking advice only B) Niacin C) Statin D) Fibrate E) More alcohol
Is Mr S.K’s his lipid disorder..... Primary Secondary
Is Mr S.K’s his lipid disorder.....The case for “primary” HDL Apo A1 deficiency absent Tangiers disease (ABC A1 defect) very low LCAT deficiency (& fish eye disease) very low Apo A1 Milano (dimer formation) very low Most secondary causes > 0.4 mmol/l
Are there any simple tests that would provide a diagnosis? Yes No
Are there any simple tests that would provide a diagnosis? The case for “no” Apo A1 deficiency absent Western or IEF if sufficient Tangiers disease (ABC A1 defect) very low Macrophge CE efflux LCAT deficiency (& fish eye disease)very low Plasma activity if sufficient Apo A1 Milano (dimer formation) very low IEF (Iso-electric focussing) Alternative proteomic and genetic techniques, but highly specialised
Which drugs can DRASTICALLY reduce HDL-C? (More than 1 possible) A) Diuretics B) Danazol C) Beta blockers D) Probocol E) Highly Active Antiretrovirals
Which drugs can DRASTICALLY reduce HDL-C? (More than 1 possibleThe case for “B” and D” J Allergy ClinImmunol. 2005 115:864-9. Adverse effects of danazol prophylaxis on the lipid profiles of patients with hereditary angioedema. Széplaki G, Varga L, Valentin S, Kleiber M, Karádi I, Romics L, Füst G, Farkas H. Probucol, a powerful antioxidant, is a CETP and SR-B1inducer that dramatically reduces HDL-C (by 20-30%). Dayspring T et al