Download
1 / 1
10 likes | 104 Views
Frequency of Asthma Education in Primary Care for the Years 2007-2010 Marquise Lee, MSCR 1 , Kevin Cross , PharmD , MSCR 1 , Wan Yu Yang, MSCR 1 , Michael Jiroutek , DrPH 1 , Beth Sutton, PhD 1 1 Campbell University College of Pharmacy & Health Sciences, Buies Creek, North Carolina.

E N D
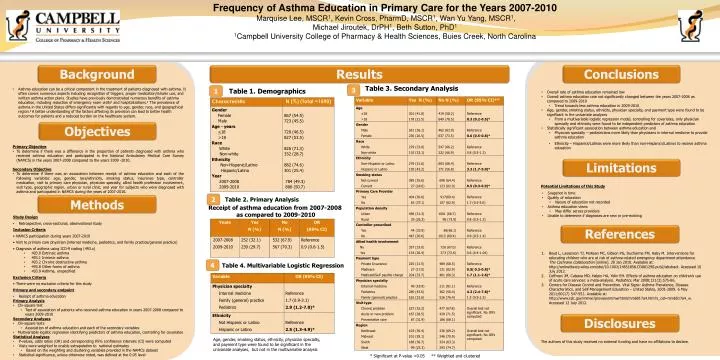
Frequency of Asthma Education in Primary Care for the Years 2007-2010 Marquise Lee, MSCR1, Kevin Cross, PharmD, MSCR1, Wan Yu Yang, MSCR1, Michael Jiroutek, DrPH1, Beth Sutton, PhD1 1Campbell University College of Pharmacy & Health Sciences, Buies Creek, North Carolina Background Results Conclusions Table 3. Secondary Analysis 3 • Overall rate of asthma education remained low • Overall asthma education rate not significantly changed between the years 2007-2008 as compared to 2009-2010 • Trend towards less asthma education in 2009-2010 • Age, gender, smoking status, ethnicity, physician specialty, and payment type were found to be significant in the univariate analyses • From a multivariable logistic regression model, controlling for covariates, only physician specialty and ethnicity were found to be independent predictors of asthma education • Statistically significant association between asthma education and • Physician specialty – pediatricians more likely than physicians in internal medicine to provide asthma education • Ethnicity – Hispanics/Latinos were more likely than non-Hispanics/Latinos to receive asthma education 1 • Asthma education can be a critical component in the treatment of patients diagnosed with asthma. It often covers numerous aspects including recognition of triggers, proper medication/inhaler use, and written asthma action plans. Studies have previously demonstrated numerous benefits of asthma education, including reduction of emergency room visits1 and hospitalizations.2 The prevalence of asthma in the United States differs significantly with regards to age, gender, race, and geographical region.3A better understanding of the factors affecting its provision can lead to better health outcomes for patients and a reduced burden on the healthcare system. Table 1. Demographics Objectives 24 randomized • Primary Objective • To determine if there was a difference in the proportion of patients diagnosed with asthma who received asthma education and participated in the National Ambulatory Medical Care Survey (NAMCS) in the years 2007-2008 compared to the years 2009 -2010. • Secondary Objective • To determine if there was an association between receipt of asthma education and each of the following variables: age, gender, race/ethnicity, smoking status, insurance type, controller medication, visit to primary care physician, physician specialty, allied health profession involvement, visit type, geographic region, urban or rural clinic, and year for subjects who were diagnosed with asthma and participated in NAMCS during the years of 2007-2010. Limitations 20 conventional Potential Limitations of this Study • Snapshot in time • Quality of education • Nature of education not recorded • Asthma education views • May differ across providers • Unable to determine if diagnoses are new or pre-existing 2 Table 2. Primary Analysis Methods Receipt of asthma education from 2007-2008 as compared to 2009-2010 • Study Design • Retrospective, cross-sectional, observational study • Inclusion Criteria • NAMCS participation during years 2007-2010 • Visit to primary care physician (internal medicine, pediatrics, and family practice/general practice) • Diagnosis of asthma using ICD-9 coding (493.x) • 493.0 Extrinsic asthma • 493.1 Intrinsic asthma • 493.2 Chronic obstructive asthma • 493.8 Other forms of asthma • 493.9 Asthma, unspecified • Exclusion Criteria • There were no exclusion criteria for this study • Primary and secondary endpoint • Receipt of asthma education • Primary Analysis • Chi-square test • Test of association of patients who received asthma education in years 2007-2008 compared to years 2009-2010 • Secondary Analyses • Chi-square tests • Association of asthma education and each of the secondary variables • Multivariable logistic regression identifying predictors of asthma education, controlling for covariates • Statistical Analyses • P-values, odds ratios (OR) and corresponding 95% confidence intervals (CI) were computed • Visits were weighted to enable extrapolation to national estimates • Based on the weighting and clustering variables provided in the NAMCS dataset • Statistical significance, unless otherwise noted, was defined at the 0.05 level References • Boyd L, Lasserson TJ, McKean MC, Gibson PG, Ducharme FM, Haby M. Interventions for educating children who are at risk of asthma-related emergency department attendance. The Cochrane Collaboration [online]. 20 Jan 2010. Available at: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001290.pub2/abstract. Accessed 10 July 2012. • Coffman JM, Cabana MD, Halpin HA, Yelin EH. Effects of asthma education on children’s use of acute care services: a meta-analysis. Pediatrics. Mar 2008;121(3):575-86. • Centers for Disease Control and Prevention. Vital Signs: Asthma Prevalence, Disease Characteristics, and Self-Management Education – United States, 2001-2009. 6 May 2011;60(17) 547-552. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6017a4.htm?s_cid=mm6017a4_w. Accessed 12 July 2012. 4 Table 4. Multivariable Logistic Regression Disclosures Age, gender, smoking status, ethnicity, physician specialty, and payment type were found to be significant in the univariate analyses, but not in the multivariable analysis The authors of this study received no external funding and have no affiliations to declare. * Significant at P-value <0.05 ** Weighted and clustered