Download
1 / 1
10 likes | 179 Views
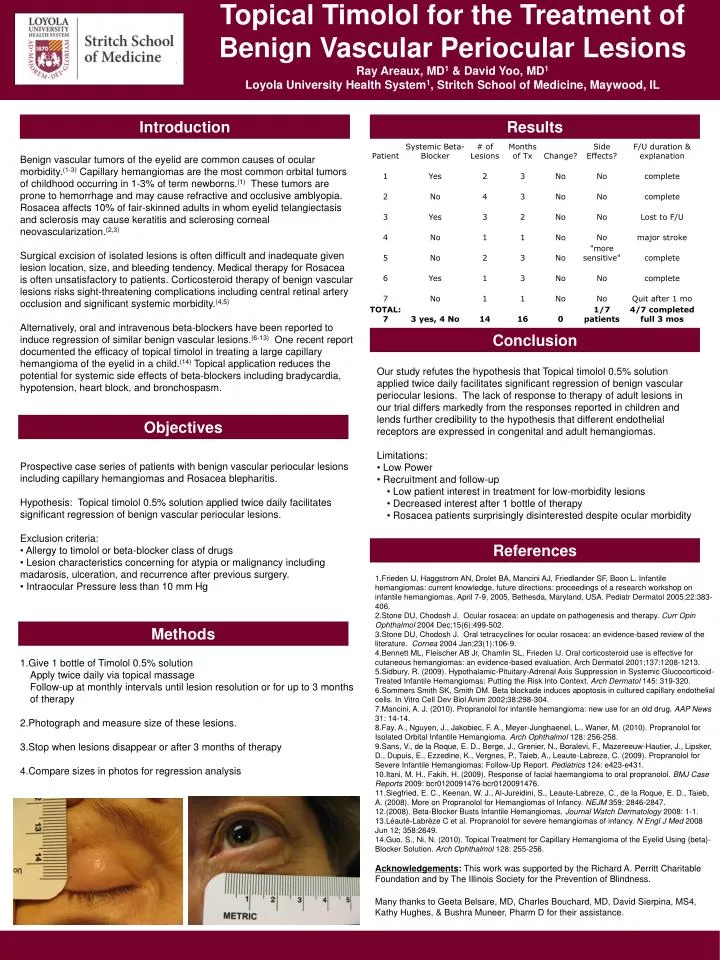
Topical Timolol for the Treatment of Benign Vascular Periocular Lesions Ray Areaux, MD 1 & David Yoo, MD 1 Loyola University Health System 1 , Stritch School of Medicine, Maywood, IL. Introduction. Results.

E N D
Topical Timolol for the Treatment of Benign Vascular Periocular Lesions Ray Areaux, MD1 & David Yoo, MD1 Loyola University Health System1, Stritch School of Medicine, Maywood, IL Introduction Results Benign vascular tumors of the eyelid are common causes of ocular morbidity.(1-3) Capillary hemangiomas are the most common orbital tumors of childhood occurring in 1-3% of term newborns.(1) These tumors are prone to hemorrhage and may cause refractive and occlusive amblyopia. Rosacea affects 10% of fair-skinned adults in whom eyelid telangiectasis and sclerosis may cause keratitis and sclerosing corneal neovascularization.(2,3) Surgical excision of isolated lesions is often difficult and inadequate given lesion location, size, and bleeding tendency. Medical therapy for Rosacea is often unsatisfactory to patients. Corticosteroid therapy of benign vascular lesions risks sight-threatening complications including central retinal artery occlusion and significant systemic morbidity.(4,5) Alternatively, oral and intravenous beta-blockers have been reported to induce regression of similar benign vascular lesions.(6-13) One recent report documented the efficacy of topical timolol in treating a large capillary hemangioma of the eyelid in a child.(14) Topical application reduces the potential for systemic side effects of beta-blockers including bradycardia, hypotension, heart block, and bronchospasm. Conclusion • Our study refutes the hypothesis that Topical timolol 0.5% solution applied twice daily facilitates significant regression of benign vascular periocular lesions. The lack of response to therapy of adult lesions in our trial differs markedly from the responses reported in children and lends further credibility to the hypothesis that different endothelial receptors are expressed in congenital and adult hemangiomas. • Limitations: • Low Power • Recruitment and follow-up • Low patient interest in treatment for low-morbidity lesions • Decreased interest after 1 bottle of therapy • Rosacea patients surprisingly disinterested despite ocular morbidity Objectives Prospective case series of patients with benign vascular periocular lesions including capillary hemangiomas and Rosacea blepharitis. Hypothesis: Topical timolol 0.5% solution applied twice daily facilitates significant regression of benign vascular periocular lesions. Exclusion criteria: • Allergy to timolol or beta-blocker class of drugs • Lesion characteristics concerning for atypia or malignancy including madarosis, ulceration, and recurrence after previous surgery. • Intraocular Pressure less than 10 mm Hg References Frieden IJ, Haggstrom AN, Drolet BA, Mancini AJ, Friedlander SF, Boon L. Infantile hemangiomas: current knowledge, future directions: proceedings of a research workshop on infantile hemangiomas, April 7-9, 2005, Bethesda, Maryland, USA. Pediatr Dermatol 2005;22:383-406. Stone DU, Chodosh J. Ocular rosacea: an update on pathogenesis and therapy. Curr Opin Ophthalmol 2004 Dec;15(6):499-502. Stone DU, Chodosh J. Oral tetracyclines for ocular rosacea: an evidence-based review of the literature. Cornea 2004 Jan;23(1):106-9. Bennett ML, Fleischer AB Jr, Chamlin SL, Frieden IJ. Oral corticosteroid use is effective for cutaneous hemangiomas: an evidence-based evaluation. Arch Dermatol 2001;137:1208-1213. Sidbury, R. (2009). Hypothalamic-Pituitary-Adrenal Axis Suppression in Systemic Glucocorticoid-Treated Infantile Hemangiomas: Putting the Risk Into Context. Arch Dermatol 145: 319-320. Sommers Smith SK, Smith DM. Beta blockade induces apoptosis in cultured capillary endothelial cells. In Vitro Cell Dev Biol Anim 2002;38:298-304. Mancini, A. J. (2010). Propranolol for infantile hemangioma: new use for an old drug. AAP News 31: 14-14. Fay, A., Nguyen, J., Jakobiec, F. A., Meyer-Junghaenel, L., Waner, M. (2010). Propranolol for Isolated Orbital Infantile Hemangioma. Arch Ophthalmol 128: 256-258. Sans, V., de la Roque, E. D., Berge, J., Grenier, N., Boralevi, F., Mazereeuw-Hautier, J., Lipsker, D., Dupuis, E., Ezzedine, K., Vergnes, P., Taieb, A., Leaute-Labreze, C. (2009). Propranolol for Severe Infantile Hemangiomas: Follow-Up Report. Pediatrics 124: e423-e431. Itani, M. H., Fakih, H. (2009). Response of facial haemangioma to oral propranolol. BMJ Case Reports 2009: bcr0120091476-bcr0120091476. Siegfried, E. C., Keenan, W. J., Al-Jureidini, S., Leaute-Labreze, C., de la Roque, E. D., Taieb, A. (2008). More on Propranolol for Hemangiomas of Infancy. NEJM 359: 2846-2847. (2008). Beta-Blocker Busts Infantile Hemangiomas. Journal Watch Dermatology 2008: 1-1. Léauté-Labrèze C et al. Propranolol for severe hemangiomas of infancy. N Engl J Med 2008 Jun 12; 358:2649. Guo, S., Ni, N. (2010). Topical Treatment for Capillary Hemangioma of the Eyelid Using {beta}-Blocker Solution. Arch Ophthalmol 128: 255-256. Acknowledgements: This work was supported by the Richard A. Perritt Charitable Foundation and by The Illinois Society for the Prevention of Blindness. Many thanks to Geeta Belsare, MD, Charles Bouchard, MD, David Sierpina, MS4, Kathy Hughes, & Bushra Muneer, Pharm D for their assistance. Methods • Give 1 bottle of Timolol 0.5% solution • Apply twice daily via topical massage • Follow-up at monthly intervals until lesion resolution or for up to 3 months of therapy • Photograph and measure size of these lesions. • Stop when lesions disappear or after 3 months of therapy • Compare sizes in photos for regression analysis