Download
1 / 30
690 likes | 2.7k Views
OUTLET OF THORAX. By- Dr Garima Sehgal. Components of thoracic cage. Thoracic vertebrae Ribs & costal cartilages Sternum. S uperior and inferior apertures of thorax. Outlet (inferior aperture) Closed by a diaphragm ?. Inlet (superior aperture) Closed by a diaphragm ?.

E N D
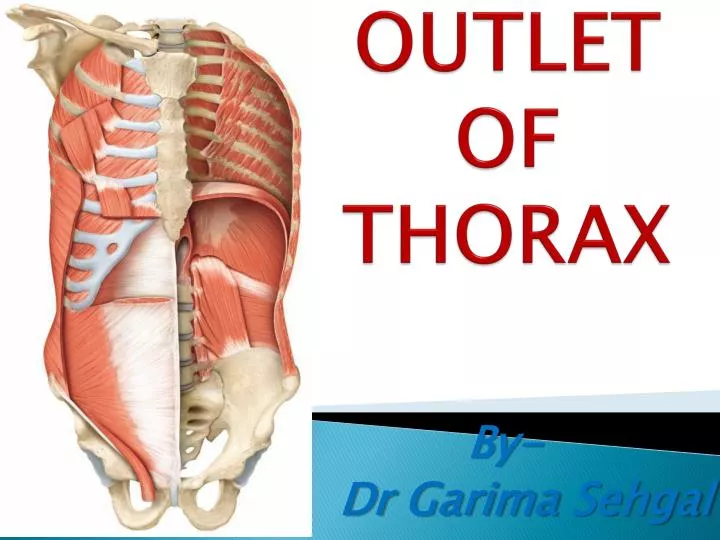
OUTLET OF THORAX By- Dr GarimaSehgal
Components of thoracic cage Thoracic vertebrae Ribs & costal cartilages Sternum
Superior and inferior apertures of thorax • Outlet (inferior aperture) • Closed by a diaphragm ? • Inlet (superior aperture) • Closed by a diaphragm ?
Attachments (Origin) –inferior view • Sternal • Costal • Lumbar
Apertures of the diaphragm • There are three large openings, 1) Aortic, 2) Oesophageal 3) Vena caval • and a number of smaller ones.
Aortic aperture osseo-aponeuroticopening • Lowest & most posterior • to the left of the midline • level -lower border of T-12 • lies behind the diaphragm Transmits aorta, thoracic duct, lymphatic trunks from the lower posterior thoracic wall and, sometimes, the azygos and hemiazygos veins
Oesophageal aperture Level T-10 in front and left of, the aortic opening is bounded by muscle fibres of the right crus. It transmits oesophagus, gastric nerves, oesophageal branches of the left gastric vessels lymphatics
Vena caval aperture Highest Level disc between T-8 & T-9 quadrilateral, and located in the central area of the tendon –so aponeurotic. traversed by – inferior vena cava and by some branches of the right phrenic nerve.
Lesser apertures • Two in each crus: one transmits the greater,otherthe lesser, splanchnic nerve. • Intercostal nerves and vessels pass in between the muscular slips of origin • Sympathetic trunks usually enter the abdominal cavity behind the medial arcuate ligament. • Subcostal nerves and vessels pass behind the • Openings for minute veins frequently occur in the central tendon
Vascular supply and lymphatic drainage • lower five intercostal& subcostal arteries • phrenic arteries • Superior phrenic • inferior phrenic • Musculophrenic • Pericardiophrenic • Superior epigastric
Phrenic veins • The right phrenic vein ends in the inferior vena cava. • The left phrenic vein is often double: one branch ends in the left renal or suprarenal vein, the other passes anterior to the oesophageal opening to join the inferior vena cava.
Phrenic nerve • two phrenic nerves • originate in the neck and pass down between the lung and heart to reach the diaphragm. • Root value (C3-C5) predominantly C4. • The phrenic nerves contain motor, sensory, and sympathetic nerve fibers.
Innervation • Motor supply - the phrenic nerves • Sensory fibres – • periphery - lower six or seven intercostal nerves • central part - Phrenic • Right crus - both right and left phrenic nerves. • crural fibres contract slightly before the costal part, and this may be functionally significant.
Phrenic nerves contd….. • Where do they pierce ? • phrenic nerve supplies the parietal pleura parietal peritoneum below, and the central diaphragm. • The trunk divides into three branches • - an anterior (sternal) branch • - anterolateral branch • - short posterior branch
Clinical importance • in avoiding surgical damage. • Thoracoabdominal incisions in a circumferential manner do not involve any significant branches of the phrenic nerves and preserve diaphragmatic function. • incisions of the central tendon are safe.
Functions of the diaphragm • is the major muscle of inspiration (67% of the vital capacity) • diaphragm lends additional power to all expulsive efforts like sneezing, coughing, laughing, crying, urinating, defaecating etc. • in lifting heavy weights. • muscular pump • Sphincter to orifice
Range of movement Diaphragmatic excursion - 1.5 cm in quiet breathing. During deep ventilation - from 6 to 10 cm. After a forced inspiration right cupola - level of T- 11 left cupola – T-12 After a forced expiration right cupola -level anteriorly with the fourth costal cartilage, laterally with the fifth, sixth and seventh ribs, and posteriorly with the eighth and the left cupola is a little lower
Development of diaphragm • Septum transversum • Pleuroperitoneal fold • Mesentry of oesophagus • Body wall
Hiatus hernia Sliding, or type I, hiatus hernia • laxity of the phreno-oesophageal membrane, allows the gastro-oesophageal junction to slide into the thorax • usually acquired, • commonly occurs in the fifth decade of life. • found in more than 50% of patients with gastro-oesophageal reflux.
Para-oesophageal, or type II, hiatus hernia • When the stomach herniates into the thorax alongside the oesophagus
Repeated stress may eventually compromise the integrity of the hiatus, so that the muscular hiatal tunnel widens. Oesophageal reflux • Reflux of gastric contents into the oesophagus, • risk of inhalation into the lungs • prevented by a physiological antireflux barrier located at the gastro-oesophageal junction • components of this barrier 1. specialized smooth muscle of the wall 2. fibres of the crura
Referred pain – pain arising from structures served by the phrenic nerve is often to other somatic regions served by spinal nerves C3-C5. (Kehr'ssign ?). • A hiccough is a spasmodic contraction of the diaphragm, which pulls air against the closed folds of the larynx. Irritation of the phrenic nerve (or the tissues supplied by it) leads to the hiccough reflex. • Patients suffering spinal cord injuries below the neck are still able to breathe effectively, despite any paralysis of the lower limbs as thephrenic nerve arises from the neck (C3-C5)
Lesions of the phrenic nerve • The phrenic nerve may be involved in • traumatic lesions of the upper brachial plexus. • Cardiac surgery • thoracic surgery, • tumours of the lung or mediastinum • infections such as typhoid and polio. • Division in the neck completely paralyses the corresponding half of the diaphragm, which atrophies. • leads to paradoxical movement of the diaphragm • best observed fluoroscopically