Download
1 / 21
210 likes | 306 Views
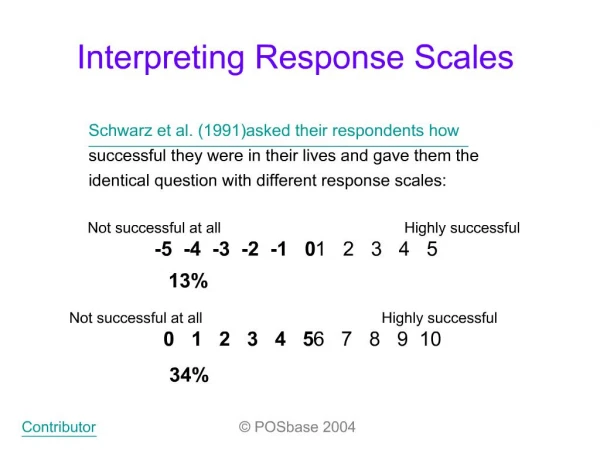
Interpreting Tumor Response. CTOS 2012, Prague. William D. Tap, MD Section Chief, Sarcoma Oncology Melanoma and Sarcoma Service Memorial Sloan-Kettering Cancer Center. Interpreting Tumor Response. Δ SUV prognostic value - ? Predictive response future chemo. Δ SUV prognostic value in ILP.

E N D
Interpreting Tumor Response CTOS 2012, Prague William D. Tap, MD Section Chief, Sarcoma Oncology Melanoma and Sarcoma Service Memorial Sloan-Kettering Cancer Center
ΔSUV prognostic value - ? Predictive response future chemo ΔSUV prognostic value in ILP Baseline SUV has predictive significance in ES, not OS; ΔSUV no correlation path necrosis/RR Path necrosis no prognostic value
pseudocapsule formation with neoadjuvant chemotherapy Path necrosis prognostic value (poorer outcomes) ? Path CR to XRT prognostic value
Important Sarcoma Community Investigator Initiated Interesting Questions and Relevant Observations Predictive + Prognostic Markers Neoadjuvant Therapy Imaging Pathology/Molecular Analysis Conundrum: In practice different degrees of acceptance Difficult incorporate findings into future studies Design trials, interpret data, validate findings
Neoadjuvant Therapy Imaging Pathology/Molecular Analysis
Neoadjuvant Therapy • Early treatment of micrometastatic disease • Theory improve DRFS and OS (Ewing’s and Osteo) • Less radiation dose and a smaller field • Improve Local Relapse Free Survival • Chemo as a radiation sensitizer • Surgical resection (smaller/necrotic dz) • ? Path necrosis surrogate marker response Very Powerful Tool in Studying and Designing Treatments for Sarcoma
Can/Do we use the data? Retrospective Phase II trials • Often low # (especially with subset analysis) • Confounders Trial Design (Regimens – XRT/chemo) • Selection Bias in Neoadjuvant Protocols • Different endpoints – LRFS, DRFS, OS, Path necrosis Numerous subgroups represented • Significant Inter subgroup heterogeneity • Significant Intra subgroup heterogeneity
WhatdoesNeoadjuvantTherapyadd to the Treatment of Sarcomas? • Tissue samples to learn about the biology of a disease • In vivo effects novel (targeted) treatments • Correlate molecular changes to treatment effects (imaging and path) • Identify prognostic and develop predictive markers • Develop insights into drug resistance • Evaluate novel imaging techniques and early assessment tools • Apply metastatic setting As a community can we design/use neoadjuvant trials to direct future cooperative studies?
Late -57% SUV Peak Early, -26% SUV Peak Responders v. Non-responders
Dead of disease 35 30 25 Recurrent / met 20 15 10 5 0 Intra and Inter Subtype Heterogeneity SUVmax in BPNST and MPNST 35 30 25 benign malignant 20 SUVmax 15 10 5 0 Patients High grade liposarcomas Courtesy of F.C. Eilber Molecular standpoint: Why differential intra and inter subtype variability Utility novel therapies (PI3K or mTOR inhibitors) Patients
EFS > 90% EFS > 98%
EURAMOS-AOST0331 X 10 weeks
RESPONSIVE LOCALIZED UNRESPONSIVE DISSEMINATED LUNG ONLY What is unique about pts with localized disease who do not respond to conventional therapy? How similar/dissimilar are they to pts who present with disseminated disease? Should we treat patients that we know are not going to respond How to introduce novel therapies
Ifosfamide Based Chemotherapy for Soft Tissue Sarcoma • n = 496 high grade, extremity STS • protocol neoadjuvant therapy • complete pathologic response (95% pathologic necrosis) • LR p= 0.001 RR 2.66 • Survival p=0.006 RR 1.86 • Ifosfamide base tx • ↑ % 95% pathologic necrosis • improved survival vs non-ifosfamide based tx p<0.001 Eilber FC et al. J Clin Oncol19:3203-3209, 2001
Conclusions: • Neoadjuvant trials critical – consensus design to direct larger studies • Imaging – Consensus directed - modality based on disease and drug • Prognostic/Predictive biomarkers critical – molecular and genetic • Validation
Treating rare diseases – what have we learned from sarcoma Weekly update: imaging sarcomas? How can the sarcoma community come to a consensus?