Download
1 / 1

E N D
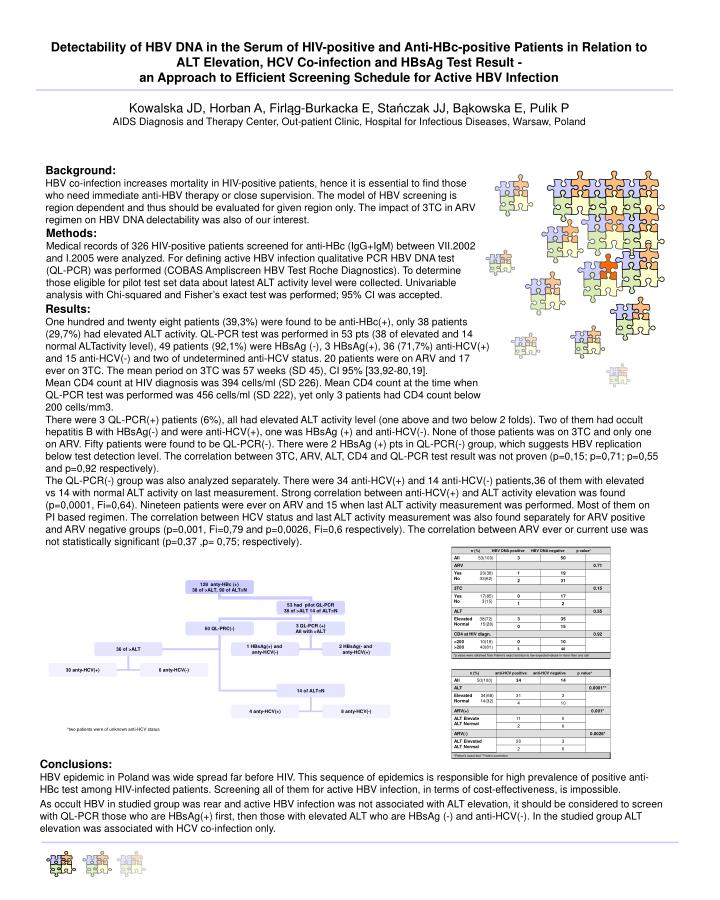
Detectability of HBV DNA in the Serum of HIV-positive and Anti-HBc-positive Patients in Relation to ALT Elevation, HCV Co-infection and HBsAg Test Result - an Approach to Efficient Screening Schedule for Active HBV InfectionKowalska JD, Horban A, Firląg-Burkacka E, Stańczak JJ, Bąkowska E, Pulik PAIDS Diagnosis and Therapy Center, Out-patient Clinic, Hospital for Infectious Diseases, Warsaw, Poland Background:HBV co-infection increases mortality in HIV-positive patients, hence it is essential to find those who need immediate anti-HBV therapy or close supervision. The model of HBV screening is region dependent and thus should be evaluated for given region only. The impact of 3TC in ARV regimen on HBV DNA delectability was also of our interest. Methods:Medical records of 326 HIV-positive patients screened for anti-HBc (IgG+IgM) between VII.2002 and I.2005 were analyzed. For defining active HBV infection qualitative PCR HBV DNA test (QL-PCR) was performed (COBAS Ampliscreen HBV Test Roche Diagnostics). To determine those eligible for pilot test set data about latest ALT activity level were collected. Univariable analysis with Chi-squared and Fisher’s exact test was performed; 95% CI was accepted. Results:One hundred and twenty eight patients (39,3%) were found to be anti-HBc(+), only 38 patients (29,7%) had elevated ALT activity. QL-PCR test was performed in 53 pts (38 of elevated and 14 normal ALTactivity level), 49 patients (92,1%) were HBsAg (-), 3 HBsAg(+), 36 (71,7%) anti-HCV(+) and 15 anti-HCV(-) and two of undetermined anti-HCV status. 20 patients were on ARV and 17 ever on 3TC. The mean period on 3TC was 57 weeks (SD 45), CI 95% [33,92-80,19]. Mean CD4 count at HIV diagnosis was 394 cells/ml (SD 226). Mean CD4 count at the time when QL-PCR test was performed was 456 cells/ml (SD 222), yet only 3 patients had CD4 count below 200 cells/mm3. There were 3 QL-PCR(+) patients (6%), all had elevated ALT activity level (one above and two below 2 folds). Two of them had occult hepatitis B with HBsAg(-) and were anti-HCV(+), one was HBsAg (+) and anti-HCV(-). None of those patients was on 3TC and only one on ARV. Fifty patients were found to be QL-PCR(-). There were 2 HBsAg (+) pts in QL-PCR(-) group, which suggests HBV replication below test detection level. The correlation between 3TC, ARV, ALT, CD4 and QL-PCR test result was not proven (p=0,15; p=0,71; p=0,55 and p=0,92 respectively). The QL-PCR(-) group was also analyzed separately. There were 34 anti-HCV(+) and 14 anti-HCV(-) patients,36 of them with elevated vs 14 with normal ALT activity on last measurement. Strong correlation between anti-HCV(+) and ALT activity elevation was found (p=0,0001, Fi=0,64). Nineteen patients were ever on ARV and 15 when last ALT activity measurement was performed. Most of them on PI based regimen. The correlation between HCV status and last ALT activity measurement was also found separately for ARV positive and ARV negative groups (p=0,001, Fi=0,79 and p=0,0026, Fi=0,6 respectively). The correlation between ARV ever or current use was not statistically significant (p=0,37 ,p= 0,75; respectively). Conclusions:HBV epidemic in Poland was wide spread far before HIV. This sequence of epidemics is responsible for high prevalence of positive anti-HBc test among HIV-infected patients. Screening all of them for active HBV infection, in terms of cost-effectiveness, is impossible. As occult HBV in studied group was rear and active HBV infection was not associated with ALT elevation, it should be considered to screen with QL-PCR those who are HBsAg(+) first, then those with elevated ALT who are HBsAg (-) and anti-HCV(-). In the studied group ALT elevation was associated with HCV co-infection only. *two patients were of unknown anti-HCV status