Download
1 / 35
350 likes | 493 Views
The Lancet and Cell Meeting What Will it Take to Achieve an AIDS-free World ? Session 4: Long term consequences of living with HIV: c omorbidities & ageing San Francisco, 3-5 November 2013.

E N D
The Lancet and Cell Meeting What Will it Take to Achieve an AIDS-free World? Session 4: Long term consequences of living with HIV: comorbidities & ageing San Francisco, 3-5 November 2013 Risk of serious disease and death in people with HIV viral suppression on ART: an epidemiologic perspective
Trend in median CD4 count in clinic populations CD4 count (/mm3) Smith C, Lampe F, Johnson M, et al
Prevalence of viral load > 50c/mL in people on ART* Proportion 2000 2005 2010 *Of those receiving ART>24 weeks Smith C, Lampe F, Johnson M, et al
Trends in death rate in people with HIV: UK Rate per 100 people Number of deaths in year Number seen for care in year Year Source: Public Health England
Trend in cause-specific death rate in people with HIV: D:A:D AIDS Other - known Liver CVD Non-AIDS cancer Unknown D:A:D unpublished
Projected life expectancy of UK man infected age 30 Nakagawa et al, AIDS 2012
What are the residual excess disease risks due to HIV in people with viral suppression ?
Cause-specific death rate in SMART/ESPRIT control arms: baseline viral load < 500 cps/mL Rate per 100 person- yrs All causes Cancer Other/ unknown Liver CVD AIDS
What are the residual excess disease risks due to HIV in people with viral suppression ? Insufficient CD4 count recovery Inflammation Adverse effects of antiretroviral drugs Note: looking at risks due to HIV and not correlates of HIV such as lifestyle factors (smoking, alcohol, recreational drug use) and mental health and hepatitis.
What are the residual excess disease risks due to HIV in people with viral suppression ? Insufficient CD4 count recovery Inflammation Adverse effects of antiretroviral drugs
CD4 count recovery on ART if fully virally suppressed UK CHIC Study; Hughes et al, HIV Medicine 2010; see also Mocroft et al Lancet 2007
Attainment of CD4 count above key thresholds in people starting ART with CD4 count < 100/mm3 with sustained virologic suppression n=400 median CD4 count at start of ART 38 /mm3 100 150 200 350 500 O’Connor et al; in revision
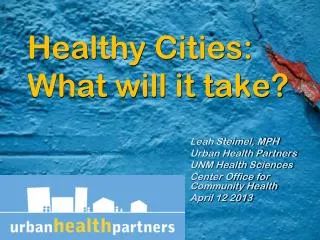
CD4 count and risk of death in people on ART with viral suppression: COHERE Most recent CD4 Death rate (/1000 person years) cell count (/mm3) Death from Death from causes any cause unrelated to HIV < 50 64.8 25.6 50 - 200 20.0 14.1 200 - 350 6.9 5.2 350 - 500 3.8 2.9 > 500 2.4 1.9 COHERE PLoS Med 2012; also Weber et al D:A:D Arch Intern Med 2006
CD4 count and risk of non-AIDS disease events in people on ART with viral suppression: D:A:D Rate ratio Liver Non-AIDS Cancer Renal Stroke MI < 200 200-349 350-499 >500 CD4 count Trend highly statistically significant in all cases except for MI Source: D:A:D (unpublished)
Natural history of HIV: CD4 count distribution according to time from infection Lodi et al; JID 2011
What are the residual excess disease risks due to HIV in people with viral suppression ? Insufficient CD4 count recovery Inflammation Adverse effects of antiretroviral drugs
Biomarker levels in SMART participants with viral load < 400 cps/mL compared with HIV negative people in CARDIA and MESA studies • People age 33-44 People age 45-75 • n fold-difference n fold-difference • IL-6 139 1.39 (p < 0.001) 291 1.60 (p < 0.001) • D-dimer ------------------------------ 293 1.49 (p < 0.001) adjusted for age, race, sex, body mass index, smoking, ratio of total cholesterol:high-density lipoprotein cholesterol, diabetes, lipid-lowering therapy, and blood pressure–lowering therapy Neuhaus et al, JID 2010
Odds ratio for elevated* IL-6 and D-dimer levels in HIV positive people on ART with viral load < 500 cps/mL compared with HIV negative people: VACS study • Odds Ratio • (95% confidence interval) • IL-6 1.04 (0.79 - 1.36) • D-dimer 0.71 (0.53 - 0.97) n ~ 1800; *elevated level is > 75th percentile adjusted for age, race/ethnicity, prevalent CVD, hypertension, diabetes, smoking, BMI, cholesterol lowering medication use, HDL, LDL, triglycerides, cocaine use in the past year, alcohol use, HCV infection, and renal disease. Armah et al, CID 2012
Baseline IL-6 / D-dimer levels and risk of serious non-AIDS and mortality in people in SMART, ESPRIT and SILCAAT control arms with viral load < 500 cps/mL n=3766 adjusted for age and sex Grund et al, CROI 2013 INSIGHT, unpublished
IL-6 and D-dimer and risk of serious non-AIDS events and death adjusted for age and sex n=3766 Grund et al, CROI 2013
What are the residual excess disease risks due to HIV in people with viral suppression ? Insufficient CD4 count recovery Inflammation Adverse effects of antiretroviral drugs
Antiretroviral drugs and risk of myocardial infarction D:A:D N Engl J Med 2003
Unanticipated association between abacavir use and raised risk of myocardial infarction D:A:D Lancet 2008
Antiretroviral drugs and renal impairment People with initial eGFR > 90 mL/min Progression to eGFR < 60 Progression to eGFR < 70 Rate ratio (95% CI) Rate ratio (95% CI) per extra year of exposure Rate ratio (95% CI) per extra year of exposure adjusted for baseline eGFR, age, sex, ethnicity, risk group, sex, nadir CD4 count, cohort, prior AIDS, baseline date, HBV, HCV, smoking, hypertension, diabetes, CVD, CD4 count, viral load, cumulative exposure to specific drugs. Ryom L et al; D:A:D CID 2013
Adjusted rate ratios for associations between ART exposure and AIDS- and non-AIDS-defining cancer AIDS-defining cancer (n = 1,151) Non-AIDS-defining cancer (n = 1,091) 1.1 1.1 1.0 1.0 aRR and 95% CI aRR and 95% CI 0.8 0.8 Any cART PI NNRTI Any cART PI NNRTI ART exposure (/year) ART exposure (/year) Adjusted for age, sex, cohort, HIV mode of acquisition, ethnic group, calendaryear, body mass index, anyprior cancer, prior AIDS diagnosis, prior AIDS cancer, smoking status, HCV and HBV status Bruyand et al D:A:D CROI 2013 Also Chao et al, AIDS 2012, Piketty et al J Clin Oncol 2012
What are the residual excess disease risks due to HIV in people with viral suppression ? Comparisons of people with high CD4 count with HIV negative populations
Comparisons of people with high CD4 count with HIV negative populations - issues with interpretation Confounding due to differences between HIV positive and HIV negative or general population comparator; e.g. smoking, drug use, socio-economic status, mental health, access to regular health care Differential ascertainment of events Selection bias within the HIV positive people; e.g. achieved viral suppression, diagnosed earlier at higher CD4 count, better health seeking behaviour, entry into a clinical trial Small relative risks correspond to large absolute risk differences at older ages
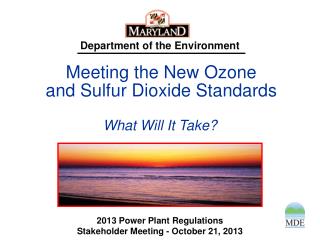
Myocardial Infarction rates compared with general population: Kaiser-Permanante database HIV +ve: 90,961 HIV –ve: 1,133,444 Relative rate95% CI p-value (compared with HIV negative) MI overall 1.4 1.3 - 1.7 <0.001 CHD overall 1.2 1.1 - 1.4 <0.001 CD4 > 500, on ART 0.9 0.8 - 1.1 0.38 CD4 > 500, not on ART 1.3 0.9 - 1.9 0.19 matched on age, sex, medical center, year of start of follow-up. Adjusted for smoking, alcohol/drug use, obesity, diabetes, lipid lowering drugs, antihypertensive drugs. Klein et al; CROI 2011
Comparison of MI risk with HIV uninfected: VACS study Hazard ratio* (95% CI) Uninfected 1.00 Infected viral load > 500 1.75 (1.40 - 2.18) Infected viral load < 500 1.39 (1.17 - 1.66) *adjusted for age, sex, race/ethnicity, hypertension, lipids, smoking, HMG-CoA reductase-inhibitor use, hepatitis C virus infection, renal disease, body mass index, and cocaine and alcohol abuse and dependence. Freiberg et al; JAMA Intern Med 2013
Death rate in ART-experienced MSM with CD4 count > 500, compared with the general population: COHERE n ~ 28,000 MSM Time with CD4 > 500 Current 1 yr Previous AIDS 2 yrs 3 yrs 4 yrs 5 yrs No previous AIDS Lewden et al, IJE 2012 See also Zwahlen et at IJE, 2009 18-39 40-59 >60 Age SMR
Survival in people on ART without risk factors compared with the general population in Denmark Estimated probability of survival from age 25 to 65 years (95% CI) General population 0.88 (0.86 - 0.90) HIV infected without 0.86 (0.77 - 0.92) HIV risk factors, comorbidities or substance abuse Obel et al, PLoS One 2011
SMR in non-IDU in SMART and ESPRIT control groups compared with the general population - Viral load < 400 and CD4 count > 350 in past 6 months CD4 350-499 CD4 > 500 SMR (95% CI) 1.771.00(1.17-2.55) (0.69-1.40) Rodger et al, AIDS 2013
Summary and Conclusions - 1 The main causes or potential causes of excess risk of serious disease due to HIV in people with viral suppression are on-going CD4 cell immunodeficency, inflammation and related factors, and adverse effects of ART. CD4 cell immunodefiency is markedly improved with virally suppressive ART but full re-normalisation can take several years and may not always be achieveable. Some excess inflammation appears to persist in people with viral suppression. Potential therapeutic approaches to enhance the rate of CD4 count restoration and/or reduce inflammation should be investigated.
Summary and Conclusions - 2 We should remain vigilant over potential adverse effects of antiretroviral drugs. Comparisons of people with high CD4 count with HIV negative people show some evidence, albeit inconsistent, for modest residual raised risk of serious clinical events and death. Interpretation is difficult and significant biases in either direction are highly possible. Nonetheless, there is sufficient evidence for excess risks, and concern that these will become more significant with ageing, that this group must remain the focus of study.
Acknowledgements Helpful comments, advice and extra analyses from: Jim Neaton Colette Smith Jason Baker Fiona Lampe Alison Rodger Caroline Sabin, Steve Deeks Amanda Mocroft David Kamara Jemma O’Connor Jacquie Neuhaus Debby Wentworth Alessandro Cozzi Lepri Jens Lundgren