Download
1 / 62
620 likes | 848 Views
Penn Cancer Center. Surgical Resection and Ablative Therapies for Hepatocellular Carcinoma. Kim M. Olthoff, MD Associate Professor of Surgery Liver Transplantation and Hepatobiliary Surgery University of Pennsylvania Philadelphia, Pennsylvania, USA.

E N D
Penn Cancer Center Surgical Resection andAblative Therapiesfor Hepatocellular Carcinoma Kim M. Olthoff, MD Associate Professor of Surgery Liver Transplantation and Hepatobiliary Surgery University of Pennsylvania Philadelphia, Pennsylvania, USA
University of Pennsylvania Medical CenterPenn Transplant Center and Cancer Center First School of Medicine in United States First Teaching Hospital in the US 2nd Nationally in NIH grand dollars
Weekly discussion of all patients with possible hepatobiliary tumors Review history and imaging Determine options for treatment Review of all pathology Determine adjuvant therapy Follow-up on cases Potential clinical trials Transplant and Hepatobiliary surgeons Surgical oncology GI surgeons Oncologists Radiologists Interventional radiologists Nuclear Medicine Hepatologists Hepatobiliary Tumor ConferenceWeekly multidisciplinary case presentations
Background:Hepatocellular carcinoma (HCC) • One of the most common fatal tumors worldwide • 80-90% of primary malignant tumors • Mostly associated with cirrhosis • Rising incidence in US due to Hepatitis C • Seen after 20 - 30 years after HCV infection • In the year 2000 - an estimated 8,000-10,000 deaths in US from HCV • Mortality rate expected to double or triple by 2015 • Much of this mortality due to development of HCC • Younger population, increasing mortality • 2-8% annual incidence of HCC in HCV cirrhosis • 5 year cumulative incidence 15-20%
Background:Natural history of HCC in cirrhosis • Prognosis – not dependent only on tumor stage • If “Resectable” • may exceed 70% 5 yr • Untreated intermediate/advanced • 10-50% 3 yr survival • Severity of disease determines outcome • Child’s A - 82% at 2 years • Child’s B/C - 36% at 2 yrs • Child’s C, large tumors • no survivors > 6 months
Cohort studies Male Advanced age HCV positivity/cirrhosis Functional impairment High AFP Other parameters Proliferation rate Irregular regeneration Dysplasia Viral genotype Columbo et al NEJM 1991 Tsukuma et al NEJM 1993 Liver Cancer Study Group Cancer 1994 Bolondi et al Gut 2001 Degos et al Gut 2000 Chen et al Int J Cancer 2002 Esnaola et al Ann Surg 2003 Tumor surveillanceDefining high risk populations
Prognosis of HCC with treatment AFP <15 associated with better outcome Fong 1999 AFP > 400 associated with poorer outcome CLIP Investigators, 2000 Prognosis of HCC Rx with OLT Pre-operative AFP not independently associated with survival Iwatsuki 2000, Shumihito 2001 AFP > 1000 RR=2.96, P=0.04 Yao, 2001 AFP > 700 Shetty, 2004 Tumor surveillance HCC and Alpha Feto-protein (AFP)
463 patients Age 40-65 Childs A or B High risk: Males > 55 HCV PT < 75% Plt < 75% 30% 2.3% Tumor surveillance Defining high and low risk populations UTZ and AFP Q 3-6 mos Velazquez et al Hepatology March 2003
Treatment of HCC“Curative” Treatment Options • Which is best? • Surgery vs. ablation? • Caveats • Only 30% of patients referred are surgical candidates • No good randomized controlled trials • Apples and oranges • Limitation of center expertise and treatment availability • Surgical resection is only proven curative treatment • Spectrum of therapy • Surgical Options: • Resection • OLT • Nonsurgical “Curative” Options: • Ablative therapies • Percutaneous Ethanol Infusion • Radiofrequency Ablation • Acetic acid Infusion
Treatment of HCCLimitations of Resection • Majority of HCC associated with cirrhosis • Reduced hepatic reserve • No accurate way to measure • Increased morbidity and mortality • Mortality now 3-10% • Surgical margins may be compromised • Multifocal tumors common • 20 to 60% of small HCC • Frequently underestimated • Recurrence rates high • 70-90% by 5 years
Surgical Resection of HCCPredictors of Recurrence • 164 patients resected for HCC (99-2001) • 55% developed recurrence with median f/u of 26 months • Median time to recurrence - 24 mos • 5 yr survival 40%, 25% RF survival • Predictors of recurrence – Univariate • Tumor > 5 cm • Multifocality • Cirrhosis (40% of patient population) • Vascular invasion • Tumor satellites • Predictors of recurrence – Multivariate • Vascular invasion Cha et al JACS 2003 MSKCC
Treatment of HCCSurgical resection and HCC in cirrhosis No Portal pressure, Bili <1 Portal pressure, Bili <1 Portal pressure, Bili 1 Patients selected by Mazzafero Criteria and Child’s A cirrhosis Llovet Hepatology 1999; 30:1434-40
Surgical Resection of HCCWho are candidates? • Best candidates • Well-compensated liver disease • Asymptomatic • Single lesion • Normal bilirubin • No evidence of portal hypertension • No medical comorbidities • Limited resection • Minimize operative time
Surgical Resection of HCCComparison between USA, France and Japan • Similar outcomes • 31-41% 5 yr survival • Larger tumors resected in US than in France or Japan • 8 cm vs. 6 and 3.5 cm • Less HCV in resection patients in US • 20% vs. 38 and 74% • Less cirrhotics resected in US • 23% vs. 52 and 65% US France Japan
Potential complications Estimated 25-30% Bleeding from coagulopathy and portal hypertension Inadequate margins Liver failure Long LOS Hospital death Recurrent disease Strategies to decrease risk Liver anesthesiologist Minimize crystalloid Transfuse FFP/plts early Keep CVP low Minimize OR time Minimize blood loss Pringle if necessary Careful post-op management Surgical Resection of HCCOperative Risks
Port Placement for Lap. left lateral segmentectomy lesion X 5 mm - working X 12 mm - Stapler 5 mm - retractor X X 12 mm - scope
Surgical Resection of HCCOutcome in US Cancer Center 78% with cirrhosis Cha et al Ann Surg 2003, 238.315 Memorial Sloan Kettering
Surgical Resection of HCCType of Resection in Transplant Eligible Patients Trisegmentectomy 2 (6%) Lobectomy Wedge/Single 8 (22%) Segment 14 (39%) Multiple Segments 12 (33%) Cha et al Ann Surg 2003, 238.315 Memorial Sloan Kettering
1.0 .8 69% Transplant Eligible N=36 .6 Survival .4 Transplant Ineligible N=144 31% .2 p=.009 0.0 0 20 40 60 80 100 Months after Resection Surgical Resection of HCCOverall Survival After Resection (N=180) Cha et al Ann Surg 2003, 238.315 Memorial Sloan Kettering
1.0 Median follow-up of 35 mos Recurrence in 20 of 36 pts .8 .6 48% RecurrenceFree Survival .4 .2 0.0 0 20 40 60 80 100 Months after Resection Surgical Resection of HCCRecurrence-Free Survival in Transplant Eligible Patients
Treatment of HCCSurgical Resection vs. OLT Three year recurrence rates 20-70% 0-43% Wong LL. Amer. J Surgery. 2002;183:309-16
Treatment of HCCSurgical Resection vs. OLTFive Year Survival 34-51% 60-69% Wong LL. Amer. J Surgery. 2002;183:309-16
Treatment of HCCAblative therapies • Direct tissue ablation • Thermal • Radiofrequency Ablation (RFA) • Cryoablation • Microwave coagulation therapy (MCT) • Laser Induced Thermotherapy (LITT) • Chemical • EtOH • Acetic acid • Chemoembolization • Radioembolization
Ablative Therapy of HCCGoals of Ablation • Equivalent to surgical resection in survival and local recurrence • Bridge therapy to stabilize disease while awaiting transplant • Palliation of unresectable, nontransplantable disease • Conversion from unresectable to resectable
Unresectable lesions Good < 3 lesions < 3 cm. Extended < 4 lesions < 5 cm. Heroic! > 4 lesions > 5 cm. Treatable under US/CT/MR guidance: Can you see it? Can you reach it? Adequate clotting function: Platelets >50K INR <1.5 Adjacent structures Bowel, gallbladder, diaphragm, vessels, bile ducts Ablative Therapy of HCCPatient Selection for RFA
Treatment of HCCAblative therapy: RFA Mechanism Coagulation Necrosis Energy Deposited Local Tissue Interactions = x - Heat Loss • Limitations for RFA: • Lesions close to heat sink make treatment less effective • Charring and impedance can limit size • Proximity of bowel or diaphragm
Ablative Therapy of HCCRFA: Technique • Percutaneous, laparoscopic, or open • Benefits and limitations of all approaches • Multiple overlapping burns to cover entire tumor volume plus “surgical margin”
Ablative Therapy of HCCRFA: Percutaneous Technique • IV access for sedation/analgesia. • No abx • 4 grounding pads • Localize lesion • Prep and local anesthetic through capsule • Puncture with RF probe to 5 mm from back wall of lesion
Ablative Therapy of HCCRFA Modality Selection:Ultrasound • Real-time guidance • Allows complex angled approach • Visualization of probe can be difficult • Steam obscures margins and probe • Imaging is inadequate endpoint for therapy
Ablative Therapy of HCCRFA Modality Selection:CT • Lesions must be conspicuous on non-contrast scans • Access limited by gantry and axial imaging • Not real-time imaging • Excellent visualization of probe location • Not obscured by steam • Can do dynamic enhanced scan to assess completion of ablation
Ablative Therapy of HCCRFA Device Selection:RITA • Radial array up to 7 cm • Measures temperature and impedance at multiple tines. • Endpoint is target temperature for a specified time. • Rise in impedance prevented by reducing power to allow complete burn time.
Ablative Therapy of HCCRFA Device Selection:Radiotherapeutics • Radial array up to 4 cm • Only measures impedance • Burn endpoint is “rolloff” of current due to rising impedance in the coagulated tissue.
OR procedure: s/p Lap. RFA R. lobe HCC Pre-Op CT Scan 3/02 3 mos post-RFA scan 6 months s/p Lap. RFA HCC Stable RFA site, NED OLTx 9 mos post-RFA, no viable tumor at RFA site, incidental 1 cm left lobe HCC 6 mos post-RFA scan
Pain Fever Vasovagal/Hypotension Oversedation Pleural Effusion (0.6%) Pneumothorax Hemorrhage (0.5%) Ascites Cholangitis Abscess Hepatic Infarct Biliary Stricture Tract Tumor Seeding Skin burns Ablative Therapies of HCCComplications of RFA
Ablative Therapies of HCCFollow-up of RFA • Imaging must be “functional” • Dynamic CT • Gad-enhanced MRI • Early arterial enhancement • Bright on T2
Ablative Therapies of HCCFollow-up of RFA: Results • “Complete” necrosis in 70-75%. • HCC 80%-90% • Local recurrence in 13%-60%. • Disease-free survival • 1 year 56% • 2 years 29% • 3 years 14% • 65% new/distant lesions Dodd GD III; Solbiati L; RSNA 2000
Ablative Therapies of HCCFollow-up of RFA vs. PEI: HCC 5 cm PEI RF • N 50 52 • # lesions 73 69 • # sessions 5.4 1.1 • 1,2 yr survival 77%,43%86%,64% • Local failure 26% 6% • Complications 0 0 Lencioni et al. Radiology 2003; 228: 235-240
Treatment of HCCExplant pathology post RFA: Methods • Patients listed for OLT at Penn • Retrospective study, between 1996-2004 • 28 patients (40 HCC) had neoadjuvant image-guided therapy 1-392 days prior to OLT • Solitary lesions: (19 pts) 2.2-5.0 cm • Multifocal HCC (9 pts) 1.1-6.0 cm diameter • Exemption to UNOS criteria: 4 patients Soulen et al 2004
Treatment of HCCExplant pathology post RFA: Methods Pathology • Viable tumor was seen in 35/40 treated nodules, but only 1 patient is completely free of tumor • 11 of the treated HCC’s had either satellite nodules or microvascular invasion • 3 patients had macroscopic extrahepatic extension or portal vein tumor thrombus, from 2 treated HCC’s and from 1 new lesion
Treatment of HCCExplant pathology post RFA: Results • 35 of the 40 treated HCC had residual viable tumor (87.5%) • 27/28 patients had viable tumor anywhere in the explanted liver at the moment of OLT (total of 55 nodules) • In 6/18 patients, imaging studies were false negative for treated and occult tumors • Recurrence-free post transplant survival is 85% with a follow-up of 1-61 months (mean 15 mos)
Treatment of HCCExplant pathology post RFA: Conclusions • Although image-guided therapy is proven to be effective to provide local control of HCC, viable local or remote tumor is identified on explanted liver in the majority of patients • Contrast enhanced follow-up CT and MRI tend to underestimate the amount of viable tumor in the treated lesions and miss additional sites of disease.
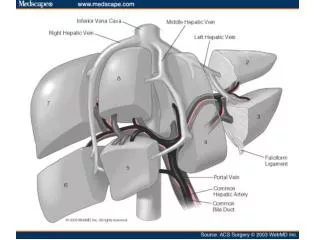
Ablative Therapy of HCCChemoembolization • Liver has a dual blood supply • Portal vein: 75-80% • Hepatic artery: 20-25% • HCC and Metastases have ~ 90% of blood supply from HA Breedis and Young, Am J Pathol 1954; 30: 969-985.
Ablative Therapy of HCCChemoembolization • No standards: • Patient selection • Number and type of embolics • Number and type of drugs • Volume of liver treated • Frequency and end-point of treatment • Measurement of response
Tissue diagnosis unless AFP>400 Unresectable disease No active extrahepatic disease No biliary obstruction No contraindication to angiography No contraindication to HA embolization hepatic failure risk >50% tumor LDH>425 AST>100 AND bili>2 Ablative Therapy of HCCChemoembolization: Eligibity at Penn
ChemoembolizationCAM-Oil-Particle 100 mg Cisplatin 50 mg Adriamycin in 8.5 cc Contrast 10 mg Mitomycin-C1.5 cc H2O emulsified with 0.1 cc/kg Ethiodol plus 150-250 µ PVA
112 Patients with HCC Majority had Hepatitis C Stratified by tumor burden and Okuda stage Patients randomized to CE, bland embolization, or supportive care CE had 2 year survival of 63% vs. 50% with bland embo and 27% with no therapy Ablative Therapy of HCCChemoembolization RCTs: Barcelona Study Llovet et al. Lancet 2002; 359: 1734-39.