Download
1 / 1
10 likes | 191 Views
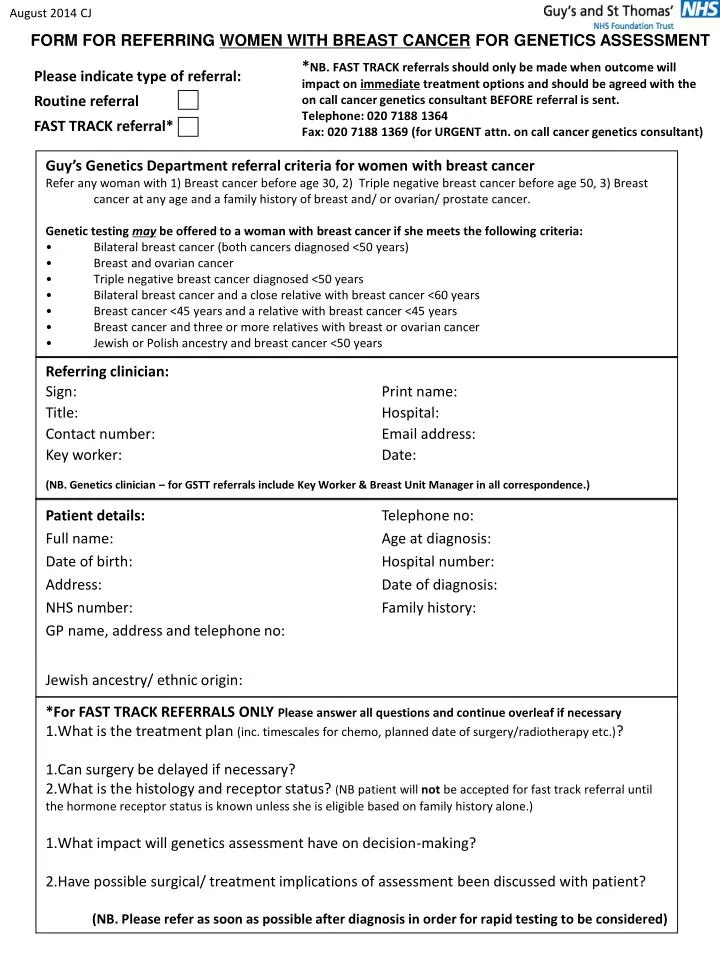
August 2014 CJ. FORM FOR REFERRING WOMEN WITH BREAST CANCER FOR GENETICS ASSESSMENT. Please indicate type of referral: Routine referral FAST TRACK referral* . * NB. FAST TRACK referrals should only be made when outcome will

E N D
August 2014 CJ FORM FOR REFERRING WOMEN WITH BREAST CANCER FOR GENETICS ASSESSMENT Please indicate type of referral:Routine referral FAST TRACK referral* *NB. FAST TRACK referrals should only be made when outcome will impact on immediate treatment options and should be agreed with the on call cancer genetics consultant BEFORE referral is sent. Telephone: 020 7188 1364 Fax: 020 7188 1369 (for URGENT attn. on call cancer genetics consultant) • Guy’s Genetics Department referral criteria for women with breast cancer • Refer any woman with 1) Breast cancer before age 30, 2) Triple negative breast cancer before age 50, 3) Breast cancer at any age and a family history of breast and/ or ovarian/ prostate cancer. • Genetic testing may be offered to a woman with breast cancer if she meets the following criteria: • Bilateral breast cancer (both cancers diagnosed <50 years) • Breast and ovarian cancer • Triple negative breast cancer diagnosed <50 years • Bilateral breast cancer and a close relative with breast cancer <60 years • Breast cancer <45 years and a relative with breast cancer <45 years • Breast cancer and three or more relatives with breast or ovarian cancer • Jewish or Polish ancestry and breast cancer <50 years Referring clinician: Sign: Print name: Title: Hospital: Contact number: Email address: Key worker: Date: (NB. Genetics clinician – for GSTT referrals include Key Worker & Breast Unit Manager in all correspondence.) Patient details: Telephone no: Full name: Age at diagnosis: Date of birth: Hospital number: Address: Date of diagnosis: NHS number: Family history: GP name, address and telephone no: Jewish ancestry/ ethnic origin: *For FAST TRACK REFERRALS ONLY Please answer all questions and continue overleaf if necessary What is the treatment plan (inc. timescales for chemo, planned date of surgery/radiotherapy etc.)? Can surgery be delayed if necessary? What is the histology and receptor status? (NB patient will not be accepted for fast track referral until the hormone receptor status is known unless she is eligible based on family history alone.) What impact will genetics assessment have on decision-making? Have possible surgical/ treatment implications of assessment been discussed with patient? (NB. Please refer as soon as possible after diagnosis in order for rapid testing to be considered)