Download
1 / 55
550 likes | 647 Views
INFLUENZA UPDATE Tuesday 8/25/09. Preface.

E N D
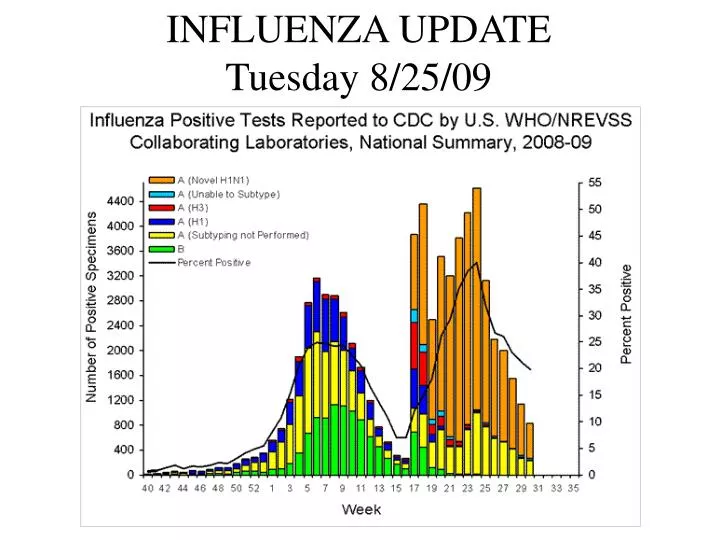
INFLUENZA UPDATE Tuesday 8/25/09
Preface This week’s update is a large one. The WHO, the CDC, and New Mexico DOH are all accelerating their preparations for the autumn influenza season. UNM has responded accordingly, activating both the UNM and the UNMH EOC’s in virtual mode; this will give us the structure to direct and facilitate our own preparedness efforts. As examples of the recent flurry of activity, this week’s update includes substantial new CDC guidance documents for colleges and universities, and for businesses; refined WHO guidelines on pharmacologic management of pandemic H1N1; and articles from BMJ, JAMA, and Inside Higher Ed. In addition to the usual updates, this document also includes brief reviews of pandemic H1N1 epidemiology, common clinical findings in hospitalized H1N1 patients, and the status of both the H1N1 and the seasonal influenza vaccine programs.
Global Updates • CDC International Situation Update 8/21/09 • Pandemic H1N1 accounts for 66% of northern hemisphere viruses and 89% of southern hemisphere viruses. • Epidemic activity appears to be declining in South and Central America, though still active in Chile , Argentina, Costa Rica, and El Salvador • Epidemic activity is declining in Europe, but remains active in the UK and Portugal. • Asia reports increasing rates of illness, especially Malaysia. Australia remains very active. • Clinical epidemiology of southern hemisphere illness is very similar to that described in the United States during spring 2009.
Pandemic lessons from Australia – BMJ 2009, 339:b3317 • Paul Torzillo, respiratory and intensive care physician, Sydney • Facilitate primary healthcare sector’s access to antiviral treatments. • Ensure primary healthcare sector is aware of obesity, pregnancy, and the postpartum period as high risk categories for severe disease. • Encourage primary healthcare sector to assess respiratory rate and where possible to do pulse oximetry in patients with typical influenza symptoms, to check for potential severe disease. • Increase intensive care capacity to cope with increased numbers of patients with overwhelming respiratory failure. • Enhance rapid delivery systems for vaccinations when available.
Pandemic lessons from Australia – BMJ 2009, 339:b3317 • Heath Kelly, head of the epidemiology unit at the Victorian Infectious Diseases Reference Laboratory • Carefully track the pandemic in order to make reasonable comparisons with past seasonal epidemics. • Have a rational approach to school closure, as has been adopted in the Australian protect phase and is planned by the US. • The messages to the public about pandemic control should be the same as for control of seasonal influenza. • Use the pandemic to improve infection control procedures in and out of hospital. • Be aware of the pandemic paradox: a high proportion of asymptomatic and mild cases but serious disease in the overweight and pregnant women. The overweight with confirmed pandemic infection may consume a disproportionate time in intensive care.
Pandemic lessons from Australia – BMJ 2009, 339:b3317 • Kate Clezy, infectious diseases physician, Sydney • Have absolutely clear infection control guidelines (many aspects have been hotly debated in Australia—eg, the merits of different types of mask, 1 m v 2 m rules for close contact, eye protection v no eye protection). • Have clear plan to manage pregnant women—from early identification, counselling, treatment, and escalation to intensive care and extracorporeal membrane oxygenation. • Have a plan to manage the workforce, especially identification and treatment of infected healthcare workers. Many will get very mild disease and would in normal circumstances continue to be at work. • Have a clear plan for communication with all staff to balance media reports with local responses. • The pandemic plans we had before A/H1N1 did not include the possibility of large numbers of people getting mildly unwell. Plans need to be reviewed to include this possibility.
Pandemic lessons from Australia – BMJ 2009, 339:b3317 • Chris Mitchell, president, Royal Australian College of General Practitioners • Patients go to their general practitioner whatever the pandemic plans say. • General practice needs the resources to meet this need. • Lack of early access to personal protective equipment and antivirals for general practice was a serious problem. • The response from general practice was reliant on the attitudes of lead general practitioners. • Variation between plans across state jurisdictions caused problems for general practice.
Should influenza immunisation for healthcare workers be mandatory? - Yes and No Last year’s British Medical Journal contains an interesting debate on the topic of mandatory influenza immunization for healthcare workers. Drs. Helms and Polgreen from the University of Iowa write in the affirmative, while Drs. Isaacs and Leask from Children’s Hospital Westmead and the University of Sydney write in the negative. The debate is attached to this email.
Two articles from JAMA 302:2 July 8, 2009 • Hospitalized patients with novel influenza A (H1N1) virus infection – California, April-May 2009 • This article was previously summarized in an update when it first appeared as CDC MMWR 2009:58:536-41. • Use of Northern Hemisphere influenza vaccines by travelers to the Southern Hemisphere • Also originally released as an MMWR, this article points out that seasonal influenza vaccines are often prepared from different selected strains in the two hemispheres, and therefore may not be equally effective in the other area. “However, this year the influenza virus strains represented in the 2008-09 northern hemisphere influenza vaccine currently available in the United States are identical to the strains represented in influenza vaccines intended for use in 2009 in the southern hemisphere.”
CDC: Distribution by age group of persons hospitalized with laboratory-confirmed influenza,* --- United States, 2007--08 winter influenza season and April 15--August 11, 2009 Note the general trend for H1N1 to affect younger people in comparison to seasonal influenza, especially the dramatic difference in persons >65 years of age.
In contrast to previous years, where the emphasis has been on seasonal influenza vaccination for those aged > 65, as seen above, for the upcoming season we are encouraging broader immunization, to reduce the overall clinical demand for ILI treatment resources.
WHO Guidelines for Pharmacological Management of Pandemic (H1N1) 2009 Influenza and other Influenza Viruses – 20 August 2009 – ATTACHED TO EMAIL
WHO Guidelines for Pharmacological Management of Pandemic (H1N1) 2009 Influenza and other Influenza Viruses – 20 August 2009 Table: Recommended Daily Dosage of Seasonal Influenza Antiviral Medications for Treatment and Chemoprophylaxis for the 2008-09 Season—United States http://www.cdc.gov/flu/professionals/antivirals/dosagetable.htm#table NB: Do not use the picture to the left. Instead , use the above link to go to the full table, which includes important qualifiers and footnotes.
World Activity by Outbreak Severity Influenza Deaths Confirmed Cases http://upload.wikimedia.org/wikipedia/commons/0/0c/H1N1_map.svg
World Activity by Outbreak Size http://en.wikipedia.org/wiki/File:H1N1_map_by_confirmed_cases.svg
Global Updates • Recent news headlines: • “ Chile finds H1N1 swine flu in turkeys” • “UAE reports first swine flu death” • “First swine flu death in Wales” • Australia: “Pandemic paradox kills few, overwhelms hospital ICUs” • “Number of A/H1N1 flu cases rises to 87 in Bangladesh” • “Athlete quarantined and tested for H1N1 virus at Canada Summer Games” • “Indonesia confirmed A/H1N1 flu cases near 1,000” • Kenya: “71 swine flu infections confirmed” • Malaysia: “257 new cases”, “569 new A(H1N1) infections” • UK: “Swine flu death toll climbs to 59” • “Vietnam’s A/H1N1 flu cases rise to 1,676”
Pandemic H1N1 Influenza Epidemiology Review • Respiratory infection with systemic effects • Transmission by respiratory secretions from an infected person • Incubation period of 1 - 5 days from exposure to symptoms • H1N1 more infectious than seasonal influenza • Infection rates: • people aged 5-24 have had the highest infection rate • median age is 12 years • people aged > 65 yo have the lowest rates • Hospitalization rates: • children < 5 yo have had the highest rates, then 5-24 yo • 71% have had an underlying medical condition • pregnant women have a 4x increase in hospitalization rates • H1N1 rates have approached or exceeded seasonal influenza rates, but are only 20% of the seasonal rate for people >65 years
Pandemic H1N1 Influenza Epidemiology Review • Community surveys spring 2009 indicated 7-10% of the population had experienced an ILI • ~ about 20% of the people in close contact with a sick person contract influenza • Outbreaks in summer camps and colleges have been common, but have been rare in nursing homes and LTCF’s • A resurgence is anticipated with the resumption of schools and universities • Medical risk factors include chronic heart, lung, renal, or liver disease; cancer; immunosuppression; pregnancy; obesity • The majority of deaths have occurred in: • 25-49 yo (42%) and 50-64 yo (28%); median age 37 • higher-risk patients (predisposing medical condition) • Circulating viruses closely resemble the H1N1 vaccine strain, and differ from the seasonal vaccine strains • Native populations may be at greater risk
H1N1 Influenza Clinical Epidemiology Review • Commonest admission Dx’s pneumonia, dehydration • Labs; ↑WBC, occ↓WBC (mean 9,500); ↑AST (median 83.5); ↑LDH; often ↑CPK (median 999); rapid H1N1 tests +/- • abnormal CXR (bilateral infiltrates c/w severe multilobar pneumonia or ARDS) • ICU admissions due to ARDS with severe hypoxemia; multiorgan dysfunction syndrome (MODS); septic shock requiring pressors; tracheostomy frequent • LOS > 30 days common • Predisposing condition, pregnancy, obesity (BMI>30-40) common in hospitalized patients • pulmonary emboli (sometimes at admission); less frequent DVT; none manifested DIC • Of patients who died, time from onset to death 17-30 days • 20 reports to WHO of oseltamivir resistance; important to keep immunocompromised patients in-house until PCR confirmation of absence of virus
H1N1 Vaccine Update/Review • single-dose syringes, multi-dose vials, inhaler sprayers • no thimerosol • first available mid-October, then weekly; latest estimates are that 45M of 195M US doses will be delivered by mid-October • initial immunizing dose, booster dose 21 days later for some • simultaneous use of inactivated-virus vaccines for H1N1 and seasonal influenza is permissible if different anatomic sites are used; simultaneous use of attenuated-live-virus vaccines for H1N1 and seasonal influenza is not recommended • Clinical trials in progress – 38 on http://clinicaltrials.gov • general population; pregnant women; adults; elderly; children; people with predisposing medical conditions • various vaccine preparations, doses, schedules; adjuvants • safety issues
H1N1 Vaccination Update/Review • CDC Guideline, Novel H1N1 Vaccination Recommendations – prioritizationif vaccine is readily available: • pregnant women • people who live with or care for children aged < 6 months • healthcare and emergency medical services personnel • people aged 6 months - 24 years • people aged 25 - 64 years with a predisposing medical condition • ~159 million people
H1N1 VaccinationUpdate/Review • prioritization if vaccine availability is limited: • pregnant women • people who live with or care for children aged < 6 months • healthcare and emergency medical services personnel who have direct contact with patients or infectious material • children aged 6 months – 4 years • children/adolescents aged 5-18 years with a predisposing medical condition • ~ 42 million people • CDC MMWR 8/21/09 – Use of Influenza A (H1N1) 2009 Monovalent Vaccine: Recommendations of the Advisory Committee on Immunization Practices, 2009
Seasonal Influenza Vaccination Update/Review • available beginning in August-September • single-dose syringes, multi-dose vials, inhaler sprayers • much broader population targeting this year because of the anticipation of a pandemic H1N1 second wave – want to reduce overall clinical burden • no pandemic H1N1 efficacy • predicted good efficacy against seasonal influenza; selected strains match circulating strains • northern hemisphere vaccines may be less effective elsewhere
Usual Priority Groups for Seasonal Influenza Vaccine • Residents and caretakers in long-term care facilities • Persons ages 2-64 years with chronic health conditions, such as: • pulmonary, cardiac, renal disease • diabetes, cancer, immunosuppression • neuromuscular disorders leading to breathing or swallowing problems • children on long-term aspirin therapy • Children age 6 months through age 18 • Persons ages 50 years and older • Pregnant women • Health care workers who provide direct patient care • Household contacts and caregivers of children up to age 5 • Anyone at increased risk of flu complications
US Updates • CDC 8/21/09: 7,983 total hospitalized cases (up 472) in 53 states and US territories (up 2), with 522 total deaths (up 45). • ME and AK report widespread activity; CA, NV, KY, NJ, GA, FL report regional activity; NM reports sporadic activity. According to CDC, any reports of widespread influenza activity in August are very unusual. • US ILI rates remain below the epidemic threshold, but are twice normal for this time of year. • 98% of all subtyped influenza strains are pandemic H1N1. • Current visits to doctors for ILI are down from April, but higher than expected for the summer months.
H1N1 in the USA by Outbreak Severity Influenza Deaths Confirmed Cases Probable Cases http://commons.wikimedia.org/wiki/File:H1N1_USA_Map.svg
Monday 5/4 Monday 5/11 Monday 5/18 Tuesday 4/28 Tuesday 5/26 Tuesday 6/2 Tuesday 6/9 Tuesday 6/16 Tuesday 6/23 Tuesday 6/30 Tuesday 7/7 Tuesday 7/14 Tuesday 7/21 Tuesday 7/28 Tuesday 8/4 Sat 8/21 Tuesday 8/11 Tuesday 8/18
H1N1 in the USA by outbreak size http://upload.wikimedia.org/wikipedia/commons/6/6c/H1N1_USA_Map_by_confirmed_cases.svg
CDC Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year • http://www.flu.gov/plan/school/higheredguidance.html • Recommendations under current flu conditions (similar to Spring 2009): • Facilitate self-isolation of residential students with flu-like illness • Those with flu-like illness should self-isolate. • Review and revise policies that make it difficult for students, faculty, and staff to stay home when they are ill or caring for a sick family member. Do not require a doctor’s note to confirm illness or recovery. • If possible, students with flu-like illness who have homes relatively close to campus should return home until recovered. • Students with a private room should remain in their room and receive care and meals from a single person. Students can establish a ‘flu buddy scheme’, and can stay in touch by e-mail, texting, or phone. • If close contact is unavoidable, sick students should be encouraged to wear a surgical mask.
CDC Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year • http://www.flu.gov/plan/school/higheredguidance.html • Recommendations under current flu conditions, continued: • Facilitate self-isolation of residential students with flu-like illness, cont. • For students who must stay on campus and who have a shared room, consider providing temporary alternate housing for students until they are recovered. • Instruct students with flu-like illness to promptly seek medical attention if they have a predisposing condition, are concerned about their illness, or develop severe symptoms. • Promote self-isolation at home by non-resident students, faculty, and staff. • Encourage these groups with flu-like illness to self-isolate at home or at a friend’s or family member’s until recovered. • Review and revise policies as indicated. Consider altering policies on absenteeism, missed classes, or late assignments. Do not require a doctor’s note to confirm illness or recovery.
CDC Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year • http://www.flu.gov/plan/school/higheredguidance.html • Recommendations under current flu conditions, continued: • Promote self-isolation at home by non-resident students, faculty, and staff. • Do not require a doctor’s note to confirm illness or recovery. • Consider increased use of distance learning or web-based education. • Provide additional information on staying home while sick. • Considerations for high-risk students and staff: • Encourage consultation with their health care provider. • Encourage vaccination. Consider a vaccination clinic. • Discourage campus visits by ill persons. • Encourage hand hygiene and respiratory etiquette. • Routine cleaning • Establish regular cleaning schedules for high-touch surfaces. • Encourage students to frequently clean their living quarters. • Provide disposable wipes for cleaning high-touch surfaces.
CDC Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year • http://www.flu.gov/plan/school/higheredguidance.html • Recommendations under current flu conditions, continued: • Considerations for specific student populations: • Review policies for students studying abroad, including access to health care and reporting illness to the university. • Determine if special communication strategies are needed to meet the needs of disabled students. • Remind health-care profession students to follow infection control guidance for health-care workers.
CDC Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year • http://www.flu.gov/plan/school/higheredguidance.html • Under conditions of INCREASED flu severity: • Permit high-risk students, faculty, and staff to stay at home during periods of high flu activity. • Plan for increased use of distance education and web-based learning. • Review policies for necessary changes – eg, withdrawal, sick leave. • Increase social distances to at least 6 feet. Consider whether to suspend large-group gatherings. • Extend the self-isolation period to 7 days or 24 hours after symptoms, whichever is longer. • Consider suspending classes. • reactively – if the university can no longer function • proactively – if spread of flu is rampant and serious • Consider whether non-residential students, faculty, and staff should restrict campus access (eg, gym or library use).
CDC Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year • http://www.flu.gov/plan/school/higheredguidance.html • Under conditions of INCREASED flu severity, continued: • Plan to be able to continue essential services (meals, custodial services, security) for residential students who cannot return home and must remain on campus (eg, international students). Facilitate departure for those who can leave. • Class suspensions would likely last at least 5-7 calendar days. Coordinate with local DOH. • Decision-making • Monitor the situation. • Make decisions in collaboration with stakeholders: • health, education, and homeland security agencies • campus staff: health, emergency management, student affairs, residential life, communications, physical plant, food services • students, staff, faculty • parents, community representatives
CDC Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year • http://www.flu.gov/plan/school/higheredguidance.html • Decision-making, continued: • Information collection and sharing • local/state health officials – trends in illness, medical visits, hospitalizations, deaths; availability of health care resources • university – absenteeism rates; visits to student health; bed availability for self-isolation; severity of illness in the university community [and nearby community] • Feasibility • Does the university have needed resources? – funds, personnel, equipment, space, time, legal authority or policy requirements, communication channels • Acceptability • Has the university considered how to address public concerns or lack of public support; secondary effects of plans (job security, financial support, educational progress).
CDC: Preparing for the Flu: A Communication Toolkit for Institutions of Higher Education http://www.flu.gov/plan/school/higheredtoolkit.html • The toolkit includes: • Questions and Answers about the CDC’s Guidance for Responses to Influenza for Institutions of Higher Education during the 2009-2010 Academic Year. • Fact Sheets for Institutions of Higher Education • Action Steps for Institutions to Prevent the Spread of Flu • Action Steps for Students, Faculty, and Staff to Protect Themselves from Flu • Poster for Institutions of Higher Education to Remind Sick People to Go Home • STOP! Do You Feel Sick? (8.5” x 11”) (PDF) (18” x 24”) (PDF ) • Template Letters (or E-mails) for Students, Faculty, Staff, and Parents • Letter to Students, Faculty, and Staff During Current Flu Conditions • Templates Announcements for Faculty, Staff, and Parents • If You are Sick with the Flu • Classes Remain in Session during Current Flu Conditions • Text Messages for Students, Faculty, Staff, and Parents • Additional Communication Resources for Institutions of Higher Education
CDC: Preparing for the Flu: A Communication Toolkit for Institutions of Higher Education http://www.flu.gov/plan/school/higheredtoolkit.html • Action Steps for Students, Faculty, and Staff to Prevent the Spread of Flu: • Practice good hand hygiene. • Cover your mouth and nose with a tissue when you cough or sneeze • Stay home or at your place of residence if you are sick for at least 24 hours after you no longer have a fever or signs of a fever. • Talk to your health care provider to find out if you should be vaccinated for seasonal flu and/or 2009 H1N1 flu. • If flu conditions become MORE severe, students, faculty, and staff should consider the following steps: • Extend the time you stay home or at your residence to at least 7 days, even if you feel better sooner. • Prepare for the possible suspension of classes by planning to continue your work at home and find a place where you can stay either by going to your home, home of a relative, or close friend of the family.
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • Key indicators for decision-making • disease severity (hospitalization rate, death rate) • extent of disease (percentage of sick people in community) • business absenteeism rate • impact of disease on employees at higher risk • other factors (eg, school dismissal) • General planning considerations • Be prepared for two scenarios – pandemic H1N1 similar to spring 2009, and influenza of increased severity • Be prepared for higher-than-normal autumn absenteeism, due to the combination of pandemic H1N1 and seasonal influenza • Work with local and state public health partners
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • General planning considerations, continued: • Keep sick workers home • Be prepared if schools or day care centers close • Actions employers should take now • Develop or update an influenza plan • Conduct a focused review of the plan to determine gaps and remaining actions • Determine your organization’s normal absenteeism rate and know how to monitor that rate for changes • Develop channels of communication to local and state public health departments • Allow sick workers to stay home without fearing job loss
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • Actions employers should take now, continued: • Develop flexible leave policies to allow workers to care for sick family members or respond to school closures • Educate your employees on your influenza plan • Share best practices within your business community • Add links to information to your company website • Important components of an influenza pandemic plan: • Develop a multi-measure, layered approach. • Identify possible work-related exposures and health risks. Reference OSHA guidelines http://www.osha.gov/dsg/topics/pandemicflu/index.html • Allow employees to stay home if they are ill, are caring for sick family members, or have children at home from school or daycare closures.
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • Important components of an influenza pandemic plan, cont: • Consider adapting policies to include flexible worksites, telecommuting, flexible work hours, and work from home. • Identify essential business functions and how to maintain them in the face of increased absenteeism. • Set up authorities, triggers, and procedures for activating and terminating the plan. • Plan to increase social distancing if directed by public health. • Establish a workforce communications plan.
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • Employer actions under current conditions (like spring 2009): • Sick persons should stay home until recovered. • expect 3-5 day absences in most cases • ensure that policies are flexible • do not require a doctor’s note • symptom-free employees with a sick family member may come to work • Sick employees at work should be advised to go home • They should self-isolate and mask until doing so. • Cover coughs and sneezes • Improve hand hygiene • Clean frequently-touched surfaces • Encourage and support employee vaccination.
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • Employer actions under current conditions, continued: • Take measures to protect employees at higher risk. • Encourage medical attention at first sign of illness. • Encourage vaccination. • Prepare for increased absenteeism. • Advice to employees on work-related travel: • Check for Sx of flu before departure and stay home if ill. • Employees who become ill should notify their supervisor and seek appropriate medical attention. • Review hygiene measures. • Overseas travelers should know how to contact the US embassy or consular office.
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • Employer actions under current conditions, continued: • Prepare for school and/or daycare closures. • Be prepared to allow workers to stay home. • Strongly recommend that parents not bring children to work. • Ensure that leave policies are flexible. • Cross-train employees in essential functions. • Employer actions if influenza severity increases: • Consider active screening of arriving employees. • Consider alternatives for higher-risk employees. • Consider increased social distancing. • Consider cancelling non-essential business travel.
CDC Guidance for Businesses and Employers to Plan and Respond to the 2009 – 2010 Influenza Season http://www.flu.gov/plan/workplaceplanning/guidance.html • Employer actions if influenza severity increases, continued: • Prepare for school and daycare closures. • Other considerations: • Some employers have stockpiled antiviral medications. See http://www.flu.gov/vaccine/antiviral_employers.html . • Identify sources of rapid, reliable information. • See the CDC Workplace Planning Toolkit http://www.flu.gov/plan/workplaceplanning/toolkit.pdf
Preparing for the Flu: A Communication Toolkit for Businesses and Employers • Questions and Answers about CDC’s Guidancefor Businesses and Employers to Plan and Respond to 2009 H1N1 Influenza • Quick Reference for Business 2009 H1N1 Flu Planning and Response • Fact Sheet for Employers - Actions Steps to Keep Your Business and Employees Healthy • Fact Sheet for Employees - 8 Ways You Can Keep Yourself Healthy • Poster for Workplace Entrances to Remind Sick Employees to Go Home • STOP! Do You Feel Sick? (8.5" x 11" PDF) (18" x 24" PDF) • Template E-mails (or Letters) for Businesses to Send to Employees • Flu Season is Starting. Get Ready Now! • If You Are Not Feeling Well . . . • Staying Healthy . . . • Text Messages for Businesses to Send to Employees • Additional Communication Resources for Businesses to Share with Employees • Additional Web Resources for Businesses to Use for Planning
“Teaching the quarantined” – Inside Higher Ed 8/19/09 “H1N1 flu may have two surprising symptoms: innovation and empathy. At least that’s the hope of University of Michigan officials, who are encouraging faculty to make broader use of technology to help sick students keep up with class work.. To that end, the university’s Center for Research on Learning and Teaching has laid out a series of guidelines to help faculty prepare for what could be a challenging year of illness…The tools Michigan faculty have been directed to use are not new. Many faculty already post PowerPoint slides online or engage in Web-based discussions. There is some expectation, however, that more faculty will gravitate toward distance-learning style instruction if flu becomes widespread on campus…While some faculty may be more resistant to showing students leniency, Winfield says contagion may prove the mother of empathy.” http://www.insidehighered.com/news/2009/08/19/flufor complete article
US Updates • Recent news headlines: • “Flu-like symptoms hit Tulane football team” • “Dolphins players test positive for H1N1” • “Kansas U students battle swine flu in first week” • “Wyoming reports first H1N1 flu death” • “Warnings over swine flu second wave” • “Marin County [CA] reports fourth swine flu death” • “Possible jail outbreak delays murder trial” • “Georgia State U swine flu rumors unfounded” • “Pregnant woman dies of swine flu in Hillsborough” • “Three cases of H1N1 reported from Hartford [OH] Fair” • “WNC youth shows resistance to flu medication” • “Duke calls off a summer program due to flu outbreak”
New Mexico updates • Wave of Sickness Hits APD Academy - More than half of the cadets training to become Albuquerque police officers are sick this week, due to an upper respiratory condition that has brought their training to a temporary halt.” ABQ Journal 8/19/09 • NM DOH to focus on priority groups first for H1N1 vaccine – “Health Secretary Alfredo Vigil, MD said today that the New Mexico Department of Health expects to begin receiving H1N1 flu vaccine as early as mid-October to protect New Mexicans against the disease…We typically receive shipments of flu vaccine in stages, which is why we vaccinate priority groups first who are most at risk for developing serious complications from the flu,” Dr. Vigil said. “We have been planning this summer for mass vaccination clinics and are well prepared for the fall flu season.” • New Mexico activity remains sporadic. DOH reports 26 hospitalizations to date in NM. Tricore Labs reported 7 cases of H1N1 in the last reporting period.