Download
1 / 28
280 likes | 391 Views
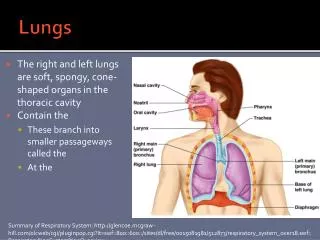
Reconditioning Donor Lungs for Transplantation Andrew Fisher. Professor of Respiratory Transplant Medicine Academic Director Institute of Transplantation Freeman Hospital, Newcastle Upon Tyne. Worldwide Adult Lung Transplants. J Heart Lung Transplant. 2012 Oct; 31(10): 1045-1095.

E N D
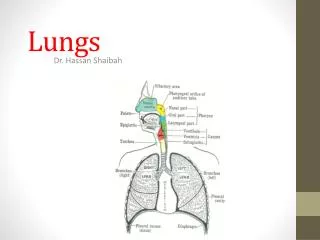
Reconditioning Donor Lungs for Transplantation Andrew Fisher Professor of Respiratory Transplant Medicine Academic Director Institute of Transplantation Freeman Hospital, Newcastle Upon Tyne
Worldwide Adult Lung Transplants J Heart Lung Transplant. 2012 Oct; 31(10): 1045-1095
Outcome of 258 UK patients listed for lung transplantation 2009-2010 31% NHS Blood and Transplant
Waiting Time to Lung Transplantby ABO blood group NHS Blood and Transplant Activity Report 2011-2012
UK Donor Utilisation for Lung Transplantation 2001-2012 Data from NHS Blood and Transplant 2012
Extended Criteria Donor Lungs Botha, Fisher et al, Transplantation 2006
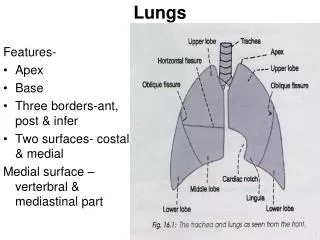
Donor Lung Assessment • Visual • Radiological • Functional • oxygenation • Physiological • haemodynamics • ventilation • metabolic • Microbiological • Biological
Objective Assessment of Donor Lung Acceptance Selection criteria poor discriminators of injury and infection leading to exclusion of potentially usable lungs. Fisher et al, Thorax 2004;59:434
Ex-Vivo Lung Perfusion Ventilator Perfusate Reservoir Reservoir Leukocyte Depleting Filter PA outflow LA inflow Pump Membrane Gas Exchanger
Professor Stig Steen Described successful reconditioning and transplantation of 6 out of 9 donor lungs deemed unusable for transplant. All 6 recipients survived the first 3 months 4 of the 6 were alive and well 12 months after transplant Ann Thorac Surg. 2009 Jan;87(1):255-60.
Establishing an EVLP Programmein Newcastle • Ethics committee approval • Hospital procedure approval • Non-clinical pilot phase • Consent of waiting list patients • Education of the transplant team • Manpower and logistics • Deciding the technique • Agreeing acceptance criteria
At start of EVLP At end of EVLP Courtesy of Ms Karen Redmond (Harefield Hospital)
Potential Impact of EVLP • Increased offering of donor organs • Increased lung transplant activity • Reduced waiting list mortality • Reduced incidence of severe PGD? • Improved longterm outcomes? • Less rejection? • Less infection? • Platform for therapeutics
Normothermic ex vivo lung perfusion in clinical lung transplantationNew England Journal of Medicine 2011; 364(15), p 1431–1440. Professor Shaf Keshavjee
Normothermic ex vivo lung perfusion in clinical lung transplantationNew England Journal of Medicine 2011; 364(15), p 1431–1440. • Phase I non-randomised safety study (n=20) • XVIVO Perfusion System • Completion date February 2010 • Outcomes in the EVLP group were comparable to that achieved with standard transplants: • 15% incidence of Primary Graft Dysfunction (PGD) in EVLP group at 72 hrs • 30% incidence of PGD in the standard transplant group • p=0.11
Commercial EVLP Systems Transmedics OCS system X-VIVO System Vivoline System
A Study of Donor Ex-vivo Lung Perfusionin United Kingdom Lung Transplantation DEVELOP-UK
Andrew Fisher Chief Investigator (Newcastle) • Karen Redmond Surgical Lead (Dublin) • Andre Simon PI (Harefield) • NizarYonan PI (Manchester) • Steven Tsui PI (Papworth) • Jorge Mascaro PI (Birmingham) • John Dark PI (Newcastle) • Nandi Marczin ITU Lead (Imperial College) Freeman Hospital DEVELOP-UK Wythenshawe Hospital Queen Elizabeth Hospital Papworth Hospital Harefield Hospital
Study Details • Design: • Non-randomised, non-inferiority observational study with an adaptive design • Funders: • NIHR Health Technology Assessment Programme and CF Trust • Sponsor: • The Newcastle upon Tyne Hospitals NHS Foundation Trust
Primary Objective: To compare survival during the first 12 months after lung transplantation in recipients of EVLP assessed and reconditioned donor lungs (treatment group) compared to that of recipients of standard donor lungs (control group), in order to assess whether survival in the EVLP treatment group over that period is non-inferior to that in the standard control group.
Secondary Objectives: • Assess early clinical outcomes • Measure quality of life (QOL) • To determine if EVLP is a cost-effective • Explore patients attitudes to and experiences of EVLP • To collect biological samples during EVLP reconditioning to support parallel mechanistic studies
Acknowledgements Newcastle EVLP Clinical Research Team Professor John Dark Dr Anders Andreasson Mr Stephen Clark Dr Mahesh Prabu Professor Paul Corris Mr Tanveer Butt Mrs Gail Johnstone Retrieval Surgeons Transplant Surgeons Transplant Co-ordinators Perfusionists Theatre Nurses Institute of Transplantation Freeman Hospital, Newcastle Upon Tyne DEVELOP-UK Thanks to all our Patients waiting for a lung transplant