Download
1 / 12
130 likes | 547 Views
Sickle Cell Anemia. Roxbury Community College ADN 253 Honors Presentation Adanna Uwandu, Shadia Laurent, Salwa Said 05/01/07. Objective. To apply the nursing process to care for patients and families with sickle cell anemia.

E N D
Sickle Cell Anemia Roxbury Community College ADN 253 Honors Presentation Adanna Uwandu, Shadia Laurent, Salwa Said 05/01/07
Objective • To apply the nursing process to care for patients and families with sickle cell anemia. • To learn the community resources available to patients and families with sickle cell anemia and sickle cell trait. • To provide care to: -individuals with the disease -individuals planning to have a family.
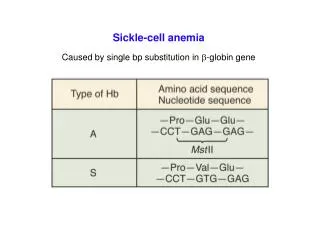
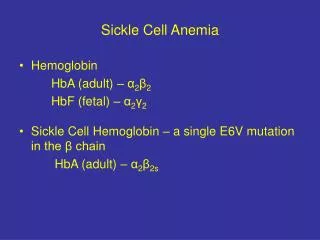
Definition of Sickle Cell Anemia • It is an autosomal recessive inherited disorder affecting the beta chain of hemoglobin • It is a congenital hematological disease. • Hemoglobin: -iron-containing portion of RBC -allows RBC to carry O2 from the lungs to tissues -normal levels in g/100mL (p.1383): *Birth; 13.7- 20.1 *3 mths 9.5-14.5 *adult levels 11-16
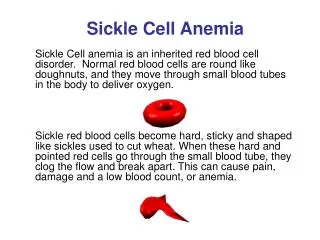
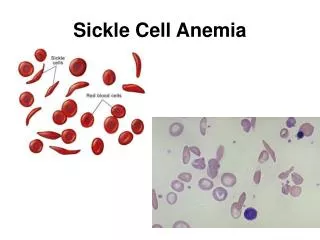
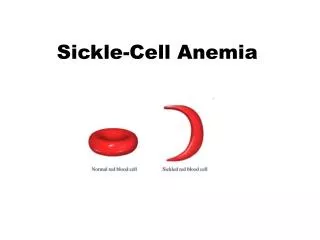
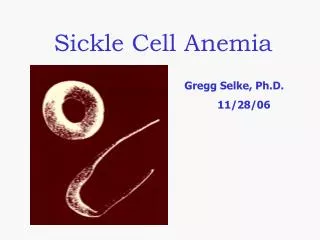
Pathophysiology • Erythrocytes (RBC) become elongated and crescent-shaped (sickled) when they are submitted to -low O2 tension/levels (< 60%-70%) -a low blood pH (acidosis) -increased blood viscosity (thick blood) • Dehydration and hypoxia can trigger these effects on the blood • Sickle cells can accumulate in capillaries and smaller blood vessels causing occlusions, impair normal circ., tissue infarctions (tissue death), swelling and anoxic changes. • Defective hemoglobin molecule is produced called Hemoglobin S.
Pathophysiology • Sickled RBC’s are thick and clump together. • RBC’s do not move freely through the blood vessels causing stasis and further sickling to occur. • Blood flow stops and the tissue distal to the blockage becomes ischemic thus causing: acute pain, cell destruction.
Fetal Hemoglobin • Is present until about six months and the child with sickle cell anemia will not usually have clinical symptoms before such time. • Fetal hemoglobin changes to adult hemoglobin around 6 mths. • Can be diagnosed in utero by • Child with sickle cell disease has hemoglobin SS, and produces no normal hemoglobin and thus shows characteristic symptoms of the disease.
Sickle Cell Trait • 25-50% of the hemoglobin produced is abnormal. • Patients who are carriers (heterozygous), can pass the gene to their offspring. • It is the benign type of SC disease. • Their normal hemoglobin outnumber the abnormal hemoglobin thus; they have
Assessment • Hemoglobin electrophoresis: few drops of blood that have converted to their adult form • Show signs ~ 6mths of disease - fever, anemia, stasis of blood and infarction > local disease. • Other signs incl: -hand-foot syndrome -slight built/thin, long arms & legs -protruding abdomen, atrophic spleen in adolescence > inc risk for infection, prophylactic antibx given
Assessment -chest syndrome ~ pneumonia occurs, enlarged liver > cirrhosis from infarctions and scarring tissue. -dec kidney function, yellowed sclerae -dec vision in children, from small retinal occlusions, regular eye exams. -priapism
Sickle Cell Crisis Definition: Sudden, severe onset of sickling. Types: sequestration crisis, aplastic crisis, megaloblastic crisis • Symptoms result from: -vaso-occlusive crisis (pooling > tissue hypoxia past the blockage point. • Triggers include: - dehydration, respiratory infection, lowered O2 exchange, dec arterial O2 level