Download
1 / 39
410 likes | 988 Views
Chapter 5 Impairment In Muscle Performance. Definitions. Strength – The maximum force that a muscle can develop during a single muscle contraction, and is the result of complex interactions of neurologic, muscular, biomechanical, and cognitive systems. Definitions (cont.).

E N D
Definitions Strength– The maximum force that a muscle can develop during a single muscle contraction, and is the result of complex interactions of neurologic, muscular, biomechanical, and cognitive systems.
Definitions (cont.) Force– Agent that produces or tends to produce a change in the state of rest or motion of an object. Kinetics – Study of forces applied to the body. Torque – The ability of a force to produce rotation. Torque = Force X Moment arm
Moment Arm Perpendicular distance from the line of action of the force to the axis of rotation. Axis Moment arm Vector of force
Torque can be altered by • Changing the force magnitude • Changing the moment arm length • Changing the angle b/t the direction of force and momentum
Power and Work Power – Rate of performing work. Work – Magnitude of force acting on an object multiplied by the distance through which the force acts. Power = Work/Time Work = Force X Distance
Endurance The ability of a muscle to sustain forces repeatedly or to generate forces over a certain period. Evaluate using: • Isometric contractions • Repeated dynamic contractions • Repeated contractions using isokinetic dynamometer
Muscle Actions • Isometric – contraction w/o motion about an axis (force is product) • Dynamic (NOT isotonic) – Concentric (shortening contraction), eccentric (lengthening contraction) • Isokinetic – Concentric or eccentric w/ constant velocity
Morphology and Physiology of Muscle Performance Improving muscle performance often translates into improvements in functioning by the patient.
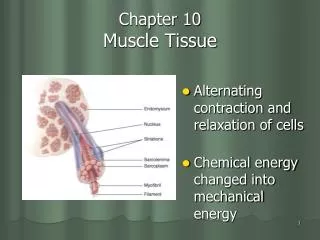
Ultrastructure of Skeletal Muscle Sarcomere – Functional unit of contractile system in muscle. A Z I H Relaxed Sarcomere Myosin Actin Titin Contracted Sarcomere
Events During Contraction and Relaxation • Depolararization of T-tubules – release of Ca2+ from SR. • Calcium binds to troponin/tropomyosin complex. • Actin combines with myosin-activated myosin ATPase. ATP splits, energy produces power stroke of X-bridges – tension is created. • ATP – binds to myosin X-bridge, allowing X-bridge to dissociate from actin.
Events During Contraction and Relaxation (cont.) 5. X-bridging activation continues as long as Ca2+ concentration is high enough to inhibit action of troponin/tropomyosin complex. 6. When stimulation ceases, Ca2+ returns to SR. 7. Removal of Ca2+ restores inhibitory action of troponin/tropomyosin. In the presence of ATP, actin and myosin remain in the relaxed state.
Muscle Fibers Strength is related to fiber diameter, not type. Type I fibers typically have smaller diameter than type II fibers.
Factors Affecting Muscle Performance 1. Fiber type 2. Fiber diameter 3. Muscle size 4. Force – velocity relationship: Active force continually adjusts to the speed at which the contractile system moves.
Length–Tension Relationship Capacity to produce force depends on the length at which muscle is held with maximum force delivered near the muscle’s normal resting length.
Muscle Architecture • The force the muscle can produce is directly proportional to the cross-sectional area (more sarcomeres in parallel). • The velocity and working excursion of the muscle are proportional to the length of the muscle (more sarcomeres in series).
More Factors Affecting Muscle Performance • Training Specificity – Muscle responds to the specific ROM, posture, type in which it’s trained. • Neurologic Adaptation – Initial increase in strength is neural adaptation (2–4 weeks). • Muscle Fatigue – Dosage of resistive exercise is limited to “form fatigue” (sacrifice of technique).
Lifespan Considerations Prepuberty • 20% of child’s body mass is muscle. • Benefits of exercise – improved muscle, motor performance, body composition, sense of well-being. • Moderate resistance training is acceptable. • Heavy resistance should be avoided. • Focus on neurologic aspects of training.
Puberty • Body composition changes to 27–40% of body mass. • Onset of puberty, strength of boys and girls diverges remarkably. • General strength training is recommended. • Avoid heavy loads (epiphyses remain vulnerable to injury).
Early Adulthood • Biologic structures are in a state of excellent adaptability. • Emphasis should be based on balanced fitness program for cardiopulmonary fitness, muscle performance, and flexibility.
Middle Age • Decrement of strength must be differentiated. • Training for as little as 2 hours per week can positively influence strength.
Advanced Age • Possible to reverse muscular weakness in old age. • Resistive exercise should be directed toward muscles susceptible to atrophic changes. • Training considerations should include power and strength.
More Factors Affecting Muscle Performance • Cognitive aspects of performance • Effects of alcohol • Effects of corticosteroids
Causes of Decreased Muscle Performance • Neurologic pathology • Muscle strain • Disuse and conditioning • Length-associated changes
Physiologic Adaptations to Resistive Training • Improvement in muscle performance • Positive effects on cardiovascular system, connective tissue, and bone Improved Functioning
Possible Physiologic Adaptations to Resistive Exercise • Muscle – in fiber size and mitochondrial density • Connective tissue – ligament and tendon strength and collagen content may • Bone – density may • Cardiovascular system – HR, systolic and diastolic BP, cardiac output and VO2 max, cholesterol
Examination and Evaluation of Muscle Performance Tests include an analysis of functional muscle strength • Manual muscle testing (consider imbalances, length–tension relationships, and positional weakness when choosing positions) • Handheld dynamometers • Isokinetic dynamometers • Dynamic strength test AND MORE
Therapeutic Exercise Intervention for Impaired Muscle Performance Enhancing performance via therapeutic exercise is at the core of the intervention program for many patients.
Activities to Increase Muscle Performance • Isometric Exercise (provides strength base for dynamic exercise) • Dynamic Exercise (weight machine exercise, free-weight exercise, plyometric exercise) • Isokinetic Exercise (provides maximum resistance throughout entire ROM)
Dosage – Intensity, Duration, Frequency, Sequence • Intensity – Perform exercise to substitution of form fatigue. • Duration – Vary rest intervals dependent upon volume (total repetitions) and rest intervals. • Frequency – Depends on rehab goals. • Sequence –Affects the development of strength. Rehab generally specific isolation training and graduate to multi-joint exercises, small-large movements.
Dosage Varies • Strength Training – 60–70% of 1RM, 8–12 reps. • Power Training – 1–3 sets 30–60% of 1RM. • Endurance Training – 10–15 reps, 10–25 reps (advanced). Shorter rest periods.
Precautions and Contraindications • Avoid use of valsalva maneuver. • Use isometrics with caution (persons at risk – high BP). • Overtraining/overwork (may lead to mood disturbances). • Caution should be used with prepubertal, pubertal children and adolescents (minimize stress to epiphyseal sites). • Acute or chronic myopathy (exercise is contraindicated).
Summary • Muscle performance = strength, power, and endurance. • Clarify when using “strength” as a qualifier in terms of force, torque, and work. • Muscle actions – static and dynamic. • Muscle morphology – thorough knowledge is needed for appropriate prescription of intervention. • Force gradation occurs by rate coding and size principles.
Summary (cont.) • Overload training – changes in hypertrophy (primarily) and hyperplasia. • Strength – must be evaluated relative to muscle length. • Specificity of training exists. • Adaptation to training – initially neurologic and precedes morphologic changes. • Form fatigue – point at which individual must discontinue exercise or sacrifice technique.
Summary – (cont.) • Resistive training – dose and goals differ. Beneficial late childhood through old age. • Impaired muscle performance – results from neurologic pathology, muscle strain, disuse, or length-associated changes. • Adaptations to resistive exercise include bone, connective tissue & cardiovascular system. • Activities to improve muscle performance – isometric, dynamic, plyometric, and isokinetic exercise.
Summary – (cont.) • Dynamic exercise may include free weights, resistive bands, pulleys, weight machines, or body weight. • Contractions during exercise include concentric, eccentric, and combinations thereof. • Dosage of exercise depends on the goal. • Precautions and contraindications must be known to ensure safety.