Download
1 / 86
860 likes | 992 Views
The Rocky Road Toward Universal Health Insurance Coverage in the USA . Fred Ralston, Jr. MD, FACP President, American College of Physicians. The past: How payment for health care has changed over the past 100 years

E N D
The Rocky Road Toward Universal HealthInsurance Coverage in the USA Fred Ralston, Jr. MD, FACP President, American College of Physicians
The past: How payment for health care has changed over the past 100 years The future: Understanding the Patient-Centered Medical Home: What Is It? What Can It Offer Patients, Physicians, and Those Paying for Health Care?
Perspective “Americans always want to do the right thing — after they have tried everything else.” Winston Churchill
Early 20th century: Teddy Roosevelt • In 1906, the American Association of Labor Legislation (AALL) initiated a campaign for national health insurance. • 1908: With support of President Roosevelt, Congress enacts first Workman’s Compensation act for civil service employees • By 1915 Workman’s Compensation laws had passed in 30 states • Health insurance coverage was considered to be the logical next step
Theodore Roosevelt Roosevelt believed that no country could be strong whose people were sick and poor 1912: Roosevelt campaigned on a platform that called for mandatory health insurance for workers
1910-1920 • 1910s: Insurance plans started to offer group coverage. Total amount of voluntary HI prior to World War I remained very small, however • Into this vacuum, compulsory HI was discussed as part of a broader Social Security movement
American Association of Labor Legislation • 1915: Bill to provide health insurance to the working class and all others that earned less than $1200 a year, including dependents • Compulsory coverage for services of physicians, nurses, and hospitals • Also provided for sick pay, maternity benefits, and death benefit for funeral expenses • Costs were to be shared between workers, employers, and the state
AALL Legislation Defeated • Supported by the AMA • Opposed by Labor • Seen as threat to unions, usurping their role in providing social benefits Samuel Gompers • Denounced by AFL leadership as an unnecessary paternalistic reform that would create a system of state supervision over people’s health • Opposed by Commercial Insurance Industry • Threat to private insurance death benefits • Lacked Popular Support
WWI -1929 • Compulsory insurance equated with German socialist insurance and Bolshevism • Increased resistance from physicians— • Viewed as threat to private practice, paternalistic, and “un-American” • Viewed as a threat to professionalism itself: mandatory fee schedules, work reviews, organizations outside the doctor-patient relationship over which doctors have no control; and limits on patient choice of physician • 1920: AMA House of Delegates opposes compulsory HI
The Great Depression and FDR • Social Security Act of 1935 provided grants for states to set up assistance programs for indigents
Franklin Delano Roosevelt • FDR spoke in favor of a right to medical care, but did not push compulsory HI over fear that it would endanger other high priority reforms: • Economic security for workers and aged, unemployment, national economic recovery, WWII • Bill after bill introduced to mandate coverage, but none passed the Congress • Growing conservative opposition to social programs after 1938
World War II • 1943: Health insurance and other worker benefits exempt from wage and price controls • 1943-49: Children’s Bureau organized a comprehensive program of maternity and infant care for military dependents; 12 million servicemen were eligible for care in hospitals and systems organized by the Armed Forces (model for the VA) • By 1944, the War Food Administration was responsible for health centers and clinics in 250 agricultural areas
1945-53: Harry Truman • 1945: Truman proposed a single plan to provide coverage for all age groups financed by 4% rise in Social Security payroll taxes
Truman Plan Fails • Union leaders advocated for insurance to protect workers from rising medical costs • But fail to enlist rank and file membership • Opposition from GOP-controlled Congress and Southern Democrats • National attention on Cold War • “Socialized medicine” made a symbolic issue in crusade against Communist influence • AMA launched massive public relations and lobbying blitz in opposition • 1946: Hill-Burton Act provides funds for hospital construction with obligation to provide free care to uninsured
1950s: Dwight Eisenhower • Eisenhower proposed to help private HI through re-insurance, regulation and initial subsidy, but no requirements on private insurance regarding how health services were provided • Tax credits for employer sponsored health insurance prompts greater private coverage • Unions winning health benefits by collective bargaining reduces their interest in seeking national legislation
1950s: Eisenhower Administration • Late 1950s: Forand bill proposed hospitalization insurance for retirees through Social Security; bill never went anywhere – opposed by Rep. Wilbur Mills, chair of the Ways and Means Committee • 1960: Kerr-Mills Act passed providing grants to states to provide need-based assistance for the elderly poor, but only 28 states participated • Federal Employee Health Benefits Program established – model for future proposals
Early 1960s: John F. Kennedy • Kennedy campaigned for a comprehensive program of HI coverage for the elderly • AMA established AMPAC with goal of electing conservatives to Congress and opposing Medicare • AMA won the propaganda war against Medicare; bill was defeated in the Senate and never got out of the House Ways and Means Committee
1960s: Lyndon B. Johnson • Assassination of JFK and LBJ’s ascendancy changed everything; LBJ believed in Medicare even more than JFK and knew how to get legislation through Congress • 1964 elections: LBJ trounced Goldwater and the Democrats gained a 2-1 majority in Congress
Medicare and Medicaid Enacted • 1965 Medicare and Medicaid passed, providing hospital and medical care for the elderly and creating a State/Federal partnership to cover the very poor
Enactment of Medicare was a Triumph of Principled Pragmatism • Key pragmatic decisions were made to ensure enactment: • Mandated hospital coverage only for the elderly • Voluntary coverage for physician services (Medicare Part B) • Payments based on “usual and customary charges” • Non-interference in practice of medicine promised • Goal was to assure the same level of care for elderly, not to attempt to change the status quo • Medicare had to pay its own way: no discounts or prospective payments; cost-based pay to hospitals
1970s: Richard Nixon • 1972: Medicare expanded to cover disabled • Wage and Price controls; beginning of limits on Medicare payments to physicians and hospitals • 1974: National Health Planning Act required “certificate of need” for new construction and acquisition of costly technology
1970s: Nixon and Ford • 1970: Sen. Ted Kennedy holds hearings and proposes single-payer plan • Sen. Long and Rep. Mills also offer plans • 1971: Nixon responds with a plan that all large employers offer catastrophic HI coverage • Nixon under threat of impeachment -- bills fail • Ford supports National HI in 1974 but later withdraws support as inflation rises • Scandal forces Rep. Mills to leave; coalitions for reform weakened, efforts again fail
Jimmy Carter • 1976: Carter campaigns for catastrophic plan • After election priority shifts to controlling health care costs; but he proposes a plan • Sen. Kennedy offers new legislation for mandatory employer HI, government subsidies for poor, competition among private plans, and negotiated fees • Bills fail due to economic recession, rising health costs, Congressional committee restructuring, and failure of advocates for comprehensive coverage to compromise
1980s: Reagan/Bush • Reagan favored repeal or overhaul of many of the regulatory laws passed in the previous decade (e.g., National Health Planning Act and PSRO program) • Market-based “pro-competition” approach and tax credits favored for expanding HI • Medicare catastrophic and prescription drug coverage enacted, but repealed as seniors objected to paying for it • Growth in federal budget deficits led to new methods of paying doctors and hospitals
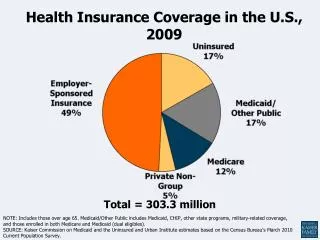
1990s: Bill Clinton • Rising health care costs and 46 million uninsured increased popular support for HI reform • Clinton administration became the first since Truman to pursue a comprehensive plan to provide universal coverage • Health Security Act called for mandated employer and individual coverage, managed competition, purchasing alliances, and global budgets • Plan fails to pass congressional committees
Late 1990s: Clinton Administration • Following defeat of Clinton plan, more modest goals were set for expanding coverage (e.g. 1997 Children’s Health Insurance Program for low-income children) • GOP take-over of Congress led to enactment of Balanced Budget Act of 1997, which mandated cuts in payments to hospitals, physicians, other providers and new “Medicare+Choice” program—first step toward goal of privatizing Medicare • In 1998, Congress replaced the VPS with the Sustainable Growth Rate (SGR).
2001-2009: George W. Bush • Prevailing conservative political view was to use “market competition” and the “purchasing power” of the federal government to reduce costs and improve quality • Key elements included: “transparency’ in pricing of services, measurement of performance, public reporting of quality and cost data to “empower” consumers, basing compensation on performance (P4P), and providing incentives for individuals to save for their own care (HSAs) with protection against catastrophic costs
2001-2009: George W. Bush • Ironically, Republican Congress passed and President George W. Bush sign into law the largest expansion of federal entitlements since 1965: Medicare Prescription Drug Program (Part D) • Decision to run the program through private insurers and PBMs put a conservative “stamp” on expansion of entitlements
2001-2009: George W. Bush • Democrats re-gained control of both the House and Senate in 2006 mid-term elections, representing a shift away from prevailing “conservative” trend • But the country, and the U.S. Senate, remained closely divided • Reauthorization fight over CHIP (2007-2008) marked by extreme partisanship
2009 – Obama Administration • Obama campaigned for universal health care coverage • 2008 elections returned the Democrats to the White House and solidified control over Congress
2010 Affordable Health Care Act Passed • Pragmatic Approach: Builds on private insurance and existing government programs • Effort made to gain support of public and interest groups • President worked with Congress • Support from labor, medicine, & business • Minimized opposition of insurers, hospitals, and drug companies • Provisions implemented gradually 2010-20 • Obama and Congressional leaders persevered
The present – an unsustainable health care delivery system that overvalues procedures and undervalues prevention and primary care Is there a way to align incentives in a way where patients, physicians and insurers want the right treatment at the right time for everyone? The Patient-Centered Medical Home: What Is It? What Can It Offer Patients, Physicians, and Those Paying for Health Care?
Two kinds of talks • Emotional – from the heart but without the data to back it up • Data filled slides that put everyone to sleep and while evidence-based are met with skepticism by those who feel they may not be relevant to those practicing in “the real world” – whether community or academia • I hope to show you why as a practicing internist I am so excited about the medical home and also that we have the data to back this up
From the heart • Internal medicine – both general and subspecialty is a highly rewarding professional career – I would argue among the highest callings possible • General internal medicine and many subspecialties face tremendous threats to survival without improved payment • Those subspecialists who like the current payment system need to know that it is unsustainable and will melt down if the cost curve is not bent
From a self-professed health policy wonk • I am convinced that there is no way possible under the current payment model to rebalance primary care through modifications to the RBRVS alone • There is no traction to pleas asking for higher payments for primary care using the current delivery model • There will be continued unfunded or semi-funded mandates or expectations involving but not limited to quality improvement and reporting
From a self-professed health policy wonk in private practice • I am sympathetic to internists who say that the patient-centered medical home is what they have been doing for twenty years • Many practices are close but require documentation and others have further to go • With current trends in workforce and practice overhead, if there is no fundamental change in payment private practice of general internal medicine will only exist in subsidized environments
Subsidized environments? • Hospital ownership of practices • Integrated groups pulling in revenue from ancillaries and other specialties • Those offering an insurance product or gain sharing with insurers • Concierge medicine
Recruiters Delight • (A) Physicians without subsidy often are barely able to meet overhead and are left with limited salaries • (B) Physicians who are paid a salary that truly reflects their contribution often receive a salary $80,000 or more in excess of those in (A) • It is easy for recruiters to do well receiving a fee moving doctors from (A) to (B)
Unintended Consequences • (A) Physicians without subsidy often are barely able to meet overhead and are left with limited salaries • (B) Physicians who are paid a salary that truly reflects their contribution often receive $80,000 or more higher than those in (A) • Doctors in (A) are often key elements of care in rural , inner city and underserved areas • This transfer of talent could further add to disparities in health care
Unintended Consequences • Smaller practices with seasoned veterans may close before they can attract new physicians to provide care • It would be wise to bring a new generation to learn the art of medicine from those who have decades of experience • Time is short • We need to increase the pipeline for primary care before these potential mentors leave practice
Alignment of incentives • Hospitals, unless the process changes from previous efforts, are not well suited to be nimble in running medical practices • Some of the first savings to be gained from improved medical practice is savings from hospital admissions – that runs counter to financial pressures on hospitals • If general internal medicine (and other primary care) is reimbursed according to its true worth rather than as a loss leader it allows us to test various models of practice organization
From someone in private practice GIM since 1983 • Revenue is flat • Less free time and more hassles • Expenses rise relentlessly • Over the years experts have regularly presented a new idea which didn’t work to save or enhance primary care
Initial response to medical home • I don’t have the time to set one up • I don’t have the money and resources to set up a medical home • It’s just another idea that will end up not working • Notice the I (or even we referring to my physician partners)
Why have I changed my mind and started to set one up? • I have been hearing great things from practices large and small who have started this process • Someone else is paying much of the start-up costs • There is a full time employee (not paid out of our limited revenue) to help us transform our practice • The patient-centered medical home will provide a platform to deal with some ongoing issues related to continuous quality improvement
Preliminary Results Indicate These Trends • Happier patients • Happier staff • Happier doctors • Lower cost • Higher quality • Helps practices do many of the things we are expected to do now but become easier in a team based approach with the proper resources
Why isn’t this just another passing fad? • Aligns incentives toward improved care • While the payment levels are not yet finalized initial levels for general internal medicine are much higher than current practice revenues allow • Best hope to provide attractive practice opportunity for new doctors • Provides proper resources to free up physicians for direct patient care • Team based approach provides opportunity to use scarce health professionals in evidence-based ways to provide cost-effective care
Why is Primary Care Important? • States with higher ratios of primary care physicians to population have better health outcomes* • Supply of primary care physicians associated with an increase in life span & reduced low birth-weight rates* • In both England and the US, each additional primary care physician per 10,000 population (a 12-20% increase) is associated with a decrease in mortality of 3-10%, depending on the cause of death** *Starfield, B., et al: The Milbank Quarterly 2005; 83:457-502 **Gulliford, J Public Health Med 2002; 24:252-4
Primary Care Associated with Decreased Costs • According to the Center for Evaluative Clinical Sciences at Dartmouth, for patients with severe chronic diseases, those who live U.S. states that relied more on primary care have: • Lower Medicare spending (inpatient reimbursements and Part B payments) • Lower resource inputs (hospital beds, ICU beds, total physician labor, primary care labor, and medical specialist labor) • Lower utilization rates (physician visits, days in ICUs, days in the hospital, and fewer patients seeing 10 or more physicians) • Better quality of care (fewer ICU deaths and a higher composite quality score Dartmouth Atlas of Health Care, Variation among States in the Management of Severe Chronic Illness, 2006
How Connected Are You to Your Primary Care Physician “Not surprisingly, those patients with the strongest relationships to specific primary care physicians were more likely to receive recommended tests and preventive care. In fact, this sense of connection with a single doctor had a greater influence on the kind of preventive care received than the patient’s age, sex, race or ethnicity.” How Connected Are You to Your Doctor? Patient–Physician Connectedness and Quality of Primary Care Steven J. Atlas, MD, MPH; Richard W. Grant, MD, MPH; Timothy G. Ferris, MD; Yuchiao Chang, PhD; and Michael J. Barry, MD 3 March 2009 | Volume 150 Issue 5 | Pages 325-335