Download
1 / 20
200 likes | 335 Views
Nervous System Manifestations of Varicella Zoster Infection Jay Panicker Jay Panicker is a specialist registrar in Neurology at the Walton Centre for Neurology and Neurosurgery . Although his primary interests are in CNS vascular diseases he retains an interest in CNS infections

E N D
Nervous System Manifestations of Varicella Zoster Infection Jay Panicker Jay Panicker is a specialist registrar in Neurology at the Walton Centre for Neurology and Neurosurgery . Although his primary interests are in CNS vascular diseases he retains an interest in CNS infections Edited by Prof Tom Solomon, Dr Agam Jung and Dr Sam Nightingale • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions This session provides an overview of nervous system manifestations of varicella zoster with particular reference to the clinical presentation, investigations, differential diagnosis and treatment options.
Learning Objectives • By the end of this session you will be able to: • Describe the spectrum of neurological syndromes associated with varicella zoster infection • Recognize the clinical presentations of the more common neurological syndromes due to varicella zoster • Outline the pathophysiology of the common CNS manifestations • Describe the investigations for CNS zoster infection • List the treatment options for various CNS manifestations • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions
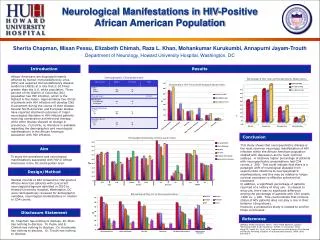
Introduction Varicella zoster (VZV) is a human α-herpesvirus. Primary infection causes chickenpox or varicella, after which it establishes latency in the cranial, dorsal root and autonomic ganglia, after which virus reactivates to cause herpes zoster. Nervous system complications can follow either primary VZV infection or reactivation of the virus. • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions Although neurological complications of primary varicella infection are rare, and those associated with reactivation are even less common, with the introduction of polymerase chain reaction (PCR) the recognised clinical spectrum of acute and chronic neurological disorders associated with VZV reactivation has widened. Above: electron micrograph of a varicella virus
Spectrum of Neurological Complications Associated with Varicella Zoster Infection . • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions
Pathophysiology of the Common Nervous System Manifestations • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions The serious manifestations arise when VZV invades the spinal cord or cerebral arteries after reactivation of the virus, causing diseases such as myelitis and focal vasculopathies. Large vessel and small vessel vasculopathies occur due to direct infection of the vessel wall and vasculitis causing thrombosis of the vessels resulting in CNS manifestations. Peripherally, nerve injury and degeneration of nociceptive neurons caused by VZV reactivation causes central sensitisation and hyperexcitablenociceptors that reduces threshold for stimuli, leading to increased excitability of central nociceptors in the dorsal horn of the spinal cord resulting in allodynia and severe pain. .
VZV Infection Without any • Cutaneous Lesions • CNS manifestations of VZV infection: • Acute Cerebellar Ataxia • Encephalitis • UnifocalVasculopathy (Large-vessel GranulomatousArteritis) Multifocal Vasculopathy (Small Vessel Arteritis) Myelitis Facial Nerve Palsy/Ramsay Hunt Syndrome Zoster Associated Pain- herpetic and Post herpetic neuralgias • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions
Acute Cerebellar Ataxia This is the most common neurological complication of primary varicella infection Onset: Typically within 1 week of the development of rash but can occur 3 days before or upto 3 weeks after Presentation. Broad based gait, nystagmus, hypotonia, slurred speech, slight nuchal rigidity CSF: Usually normal but a mild pleocytosis and raised protein can occur in upto 25% Duration: Disease usually lasts 2-4 weeks but can be as short as 3 days of as long as several months. Prognosis: Complete recovery is the norm but cerebellar deficits may persist in some cases. • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions
VZV Encephalitis • This can cause meningitis or encephalitis. It is reported to affect 0.1–0.2% of patients with VZV infection. • Patients present with: • Headache • Fever • Altered levels of consciousness • Vomiting • Mental changes • Seizures • VZV DNA is detected in arteries of both the anterior and posterior circulation but not in the brain substance suggesting VZV encephalitis is a vasculopathy that affects large and small vessels. • Large vessel disease: called unifocal vasculopathy/ granulomatous arteritis occurs mainly in immunocompetent patients and has an acute onset • Small vessel disease: multifocal vasculopathy occurs in the immunocompromised patient and has subacute presentation with varied clinical presentation • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions
VZV-related UnifocalVasculopathy (Large-vessel Granulomatous Arteritis) • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions This occurs mainly in immunocompetent elderly, but may occur at any age. Presentation: It presents as an acute focal deficit that develops weeks to months after contralateral trigeminal distribution of herpes zoster. It may be monophasic and self limiting but can be remitting or progressive with a mortality rate of up to 25%. It can also present as a stroke due to infarction in the area of brain supplied by the vessel. Angiography: Angiography reveals constriction and narrowing in the middle and anterior cerebral arteries in individuals with stroke. Occlusion of the retinal vessel or posterior circulation can occur. Onset of unifocal vasculopathy: Typical onset is 7 weeks after the development of herpes zoster, although is can occur upto 6 months after infection Mortality: 20-25% high probability of neurological sequalae
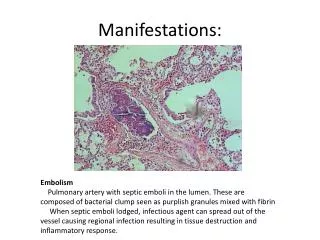
VZV-related Multifocal Vasculopathy (Small Vessel Arteritis) • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions • This usually occurs in immunocompromised patients, such as in organ transplant patients or those with a history of cancer or HIV/AIDS. • It can occur without a recent rash (30-40%) even though many cases may have history of herpes Zoster weeks before • Onset is subacute and manifests as: • Hemiplegia • Aphasia • Visual field defects • Focal deficits • It may also present with • Headaches • Fever • Altered state of consciousness • Vomiting • Seizures • CSF: may be normal or show mononuclear pleiocytosis or slightly raised protein. Tests for VSV DNA and anti VZV immunoglobulin are positive • MRI: MRI imaging reveals multiple ischemic or haemorrhagic infarcts (often both) of the cortex and subcortical white and grey matter.
VZV-related Myelitis • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions Myelitis is an uncommon neurological complication of Herpes zoster, occurring in less than 1 per 1000 cases. Neuronal and glial direct infection, vasculitis and ischaemic necrosis and immune-mediated demyelination have been proposed as mechanisms of its pathogenesis. Symptoms appear from days to weeks after the appearance of rash; they include paraparesis, dissociated or segmental sensory loss and sphincter disturbances. Clinical outcomes range from complete recovery to death. It can also present with Transverse myelitis, Brown-Séquard syndrome and ascending myelitis. An MRI may show T2 hyperintense lesions and CSF examination may show lymphocytes with raised protein, but PCR for viral DNA and VZV antibodies are positive.
Facial Nerve Palsy/Ramsay Hunt Syndrome • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions Herpes zoster reactivation involving the seventh cranial (facial) nerve causes herpes zoster oticus or Ramsay Hunt syndrome. Presents as unilateral facial weakness accompanied by a vesicular rash in the external ear canal, auricle and tympanic membrane but rarely involving the hard palate or tongue Can also present with sensorineural hearing loss, tinnitus and vertigo. Pain can occur in the absence of a typical rash and is also called zoster sine herpete
Zoster Associated Pain-herpetic and Post Herpetic Neuralgias I • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions • Acute Herpetic Neuralgia • Acute herpetic neuralgia is defined as the pain from onset of prodrome to 30 days and post herpetic neuralgia is pain persisting beyond 4 months from onset of the prodrome of herpes zoster and subacute neuralgia the pain in intervening period. • In the majority of patients, herpes zoster rash is preceded by a prodrome of dermatomal pain that is accompanied by burning, numbness or tingling and presence of prodrome increases the risk of subsequently developing more severe acute zoster pain and PHN. • Severe, acute zoster pain accompanying rash occurs in 60–90% of immuno-competent individuals with fewer than 20% of those aged <20 years and more than 80% of those aged >80 years experiencing this pain. • Allodynia (pain evoked by the application of a mild, normally non-noxious stimulus) is common in acute herpes zoster.
Zoster Associated Pain-herpetic and Post Herpetic Neuralgias II • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions • Post Herpetic Neuralgia • It is the most frequently reported complication of herpes zoster occuring in 10%of patients. It is the debilitating chronic pain that persists, in some individuals, for many months or years after the herpes zoster rash has healed and is more prevalent in the elderly. • It is characterized by constant or intermittent burning, itching or aching, with or without paroxysmal or lancinating pain. • Secondary characteristics of PHN include sleep disturbance, anorexia and weight loss, chronic fatigue and depression. Risk factors that predispose to the onset of Post herpetic Neuralgia include older age, female sex, presence of a prodrome, greater rash severity and greater acute pain severity. • Subacute herpetic neuralgia that does not progress to Post Herpetic Neuralgia reflects peripheral tissue damage and inflammation caused by a particularly severe or widespread rash.
CNS Manifestations of Varicella Investigations • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions Investigations for VZV with CNS manifestations are outlined in the table below:
The Treatment of CNS Manifestations of Varicella Zoster • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions Treatments for VZV with CNS manifestations are outlined in the table below:
Treatment of PNS Manifestations of Varicella • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions Treatments for Ramsay Hunt syndrome and herpetic/post herpetic neuralgia are outline in the table below:
Key Points • Primary infection with VZV causes varicella; reactivation of the virus manifests as herpes zoster • After reactivation of the virus, VZV occasionally invades the spinal cord or cerebral arteries, producing more severe neurological manifestations such as VZV-related myelitis or focal vasculopathies • Neurological disorders may also develop in the absence of rash • VZV-related unifocal vasculopathy (large-vessel granulomatous arteritis) is usually seen in immunocompetent elderly individuals, whereas VZV-related multifocal vasculopathy (small-vessel vasculopathy) is mostly observed in immunocompromised individuals and is often protracted • The presence of anti-VZV antibody in CSF is strongly presumptive of VZV involvement, even in the absence of PCR-amplifiable VZV DNA • Early diagnosis of more serious CNS and peripheral nervous system complications of VZV reactivation is important, as aggressive treatment with intravenous aciclovir can result in clinical benefit • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions
Summary • Learning Objectives • Having completed this session you will now be able to: • Describe the spectrum of neurological syndromes associated with varicella zoster infection • Recognize the clinical presentations of the more common neurological syndromes due to varicella zoster • Outline the pathophysiology of the common CNS manifestations • Describe the investigations for CNS zoster • List the treatment options for various CNS manifestations • Further Reading • 1. Varicella Zoster Virus and CNS Syndromes • Herpes 11 Supplement 2 2004. • 2. Zoster-associated Pain: What is known, Who is at Risk and How can it be Managed; Herpes 14 Supplement 2 2007. • 3. Severe Complications of Herpes Zoster • Herpes 14 Supplement 2 2007. • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions
Question 1 Answer the following question by clicking on either true or false. • Neurological manifestations of VSV Infections • Learning Objectives • Introduction • Neurological complications of VZV • Pathophysiology • VSV without cutaneous lesions • Acute cerbellar ataxia • VZV encephalitis • VSV related unifocal vasculopathy • VZV myelitis • Ramsay hunt syndrome • Post herpetic neuralgia • Investigations • Treatment • Key Points • Summary • Questions Varicella can cause CNS manifestations by direct vascular invasion TRUE FALSE