Download
1 / 1
10 likes | 128 Views
Do coping strategies & control beliefs change with rehabilitation? The role of neurocognition in the relationship between psychosocial and sociocognitive functioning in severe mental illness.

E N D
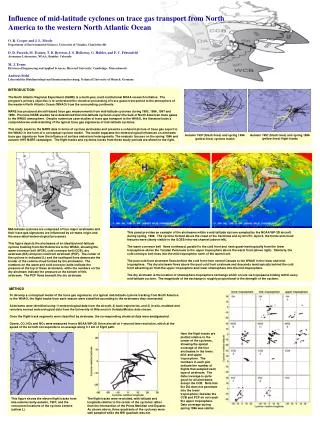
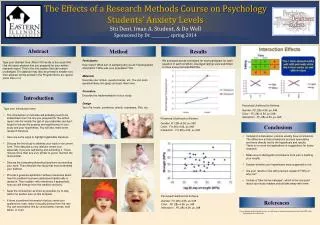
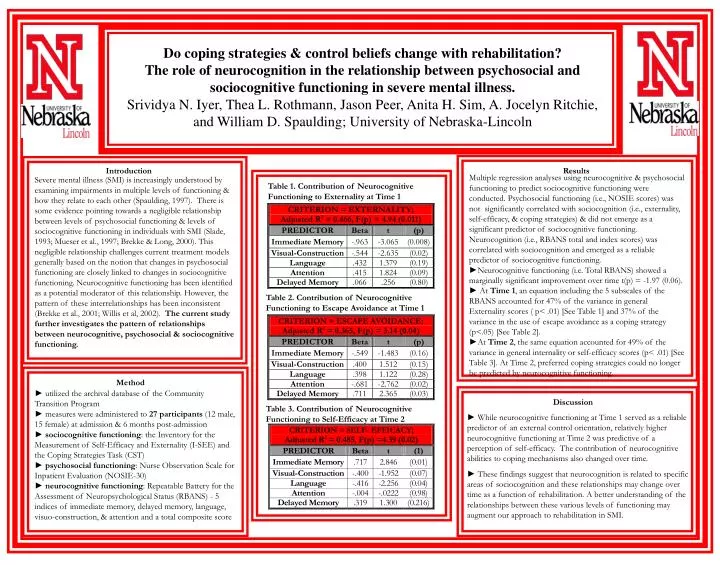
Do coping strategies & control beliefs change with rehabilitation? The role of neurocognition in the relationship between psychosocial and sociocognitive functioning in severe mental illness. Srividya N. Iyer, Thea L. Rothmann, Jason Peer, Anita H. Sim, A. Jocelyn Ritchie, and William D. Spaulding; University of Nebraska-Lincoln Introduction Results Multiple regression analyses using neurocognitive & psychosocial functioning to predict sociocognitive functioning were conducted. Psychosocial functioning (i.e., NOSIE scores) was not significantly correlated with sociocognition (i.e., externality, self-efficacy, & coping strategies) & did not emerge as a significant predictor of sociocognitive functioning. Neurocognition (i.e., RBANS total and index scores) was correlated with sociocognition and emerged as a reliable predictor of sociocognitive functioning. ►Neurocognitive functioning (i.e. Total RBANS) showed a marginally significant improvement over time t(p) = -1.97 (0.06). ►At Time 1, an equation including the 5 subscales of the RBANS accounted for 47% of the variance in general Externality scores ( p< .01) [See Table 1] and 37% of the variance in the use of escape avoidance as a coping strategy (p<.05) [See Table 2]. ►At Time 2, the same equation accounted for 49% of the variance in general internality or self-efficacy scores (p< .01) [See Table 3]. At Time 2, preferred coping strategies could no longer be predicted by neurocognitive functioning. Severe mental illness (SMI) is increasingly understood by examining impairments in multiple levels of functioning & how they relate to each other (Spaulding, 1997). There is some evidence pointing towards a negligible relationship between levels of psychosocial functioning & levels of sociocognitive functioning in individuals with SMI (Slade, 1993; Mueser et al., 1997; Brekke & Long, 2000). This negligible relationship challenges current treatment models generally based on the notion that changes in psychosocial functioning are closely linked to changes in sociocognitive functioning. Neurocognitive functioning has been identified as a potential moderator of this relationship. However, the pattern of these interrelationships has been inconsistent (Brekke et al., 2001; Willis et al, 2002). The current study further investigates the pattern of relationships between neurocognitive, psychosocial & sociocognitive functioning. Table 1. Contribution of Neurocognitive Functioning to Externality at Time 1 Table 2. Contribution of Neurocognitive Functioning to Escape Avoidance at Time 1 • ► utilized the archival database of the Community Transition Program • ►measures were administered to 27 participants (12 male, 15 female) at admission & 6 months post-admission • ►sociocognitive functioning: the Inventory for the Measurement of Self-Efficacy and Externality (I-SEE) and the Coping Strategies Task (CST) • ►psychosocial functioning: Nurse Observation Scale for Inpatient Evaluation (NOSIE-30) • ► neurocognitive functioning: Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) - 5 indices of immediate memory, delayed memory, language, visuo-construction, & attention and a total composite score Method Discussion Table 3. Contribution of Neurocognitive Functioning to Self-Efficacy at Time 2 ► While neurocognitive functioning at Time 1 served as a reliable predictor of an external control orientation, relatively higher neurocognitive functioning at Time 2 was predictive of a perception of self-efficacy. The contribution of neurocognitive abilities to coping mechanisms also changed over time. ► These findings suggest that neurocognition is related to specific areas of sociocognition and these relationships may change over time as a function of rehabilitation. A better understanding of the relationships between these various levels of functioning may augment our approach to rehabilitation in SMI.