Download
1 / 14
160 likes | 434 Views
Chapter 5. Children with Intellectual and Developmental Disabilities (IDD). Historical Overview.

E N D
Chapter 5 Children with Intellectual and Developmental Disabilities (IDD)
Historical Overview One of the first documented attempts to help children with intellectual and development disabilities (IDD) involved Jean Itard, a French physician, who tried to educate a young boy who had lived by himself in the woods—the so-called Wild Boy of Aveyron. Maria Montessori (1912) also worked in this field and developed what is now called sense training. Her work is used today with young children without disabilities in the Montessori schools.
The key organization is this area has changed its name from American Association on Mental Retardation to American Association on Intellectual and Developmental Disabilities (AAIDD) to reflect the change from “mental retardation” to “intellectual and developmental disabilities.” The main reason for the change was to try and eliminate some of the negative connotations attached to the term mental retardation.
Definition of Intellectual and Developmentally Disabilities • IDD is a disability characterized by significant limitations both in intellectual functioning and in adaptive behavior as expressed in conceptual, social, and practical adaptive skills. The disability originates before age 18. • Average IQ: 100 (average)with a range 91 to 109 • MR/IDD starts at below 70 • IDD is only 2% of the population Source: From American Association on Mental Retardation (2002). Reprinted with permission.
FIVE ASSUMPTIONS ESSENTIAL TO THE APPLICATION OF THE DEFINITION: • Limitations in present functioning must be considered within the context of community environments typical of the individual’s age peers and culture. • Valid assessment considers cultural and linguistic diversity as well as differences in communication, sensory, motor, and behavioral factors. • Within an individual, limitations often coexist with strengths. • An important purpose of describing limitations is to develop a profile of needed supports. • With appropriate personalized supports over a sustained period, the life functioning of the person with mental retardation generally will improve. • Source: From American Association on Mental Retardation (2002). Reprinted with permission.
Assessment of IDD • Intelligence tests measure the specific skills in which children with IDD differ, namely, in using memory skills, in associating and classifying information, in reasoning, and in making sound judgments. • Adaptive skills test. To be considered to have IDD, a person must be significantly deficient in adaptive behavior as expressed in conceptual skills, social skills, and practical skills. Please see Table 5.2 for more details on the categories of adaptive behaviors.
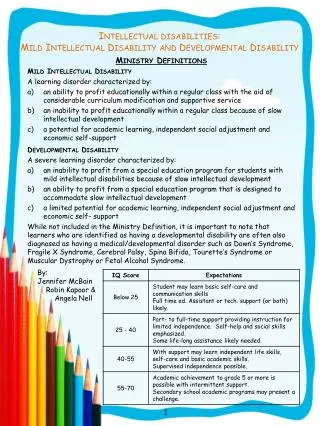
Intensity of Support • Intermittent refers to support as needed, but not necessarily present at all times. • Limited refers to support provided on a regular basis for a short period of time. • Extensive support indicates ongoing and regular involvement. • The pervasive level of support describes constant high-intensity help provided across environments and involving more staff members than the other categories.
Etiological factors • Genetic factors : Down syndrome ,normal growth and development in the embryo and fetus depend on the production of enzymes at the right time and place, PKU, fragile X syndrome—so named because of a constriction near the end of the X chromosome. • Infections: Rubella (German measles), if contracted by a woman during her first trimester of pregnancy, can result in a child with IDD. There also seems to be some evidence that children with HIV infection may develop IDD. Children and adults are also at risk of brain damage from viruses that produce high fevers, which in turn destroy brain cells. Encephalitis is one virus of this type. • Environmental factors: teratogens: substances that adversely affect fetal development: Fetal alcohol syndrome (FAS) of moderate or severe organic IDD. Lead poisoning.
Characteristics of Students with IDD • Ability to process information • Ability to acquire and use language • Ability to acquire emotional and social skills • Many children with IDD have problems in central processing, the classification of a stimulus through the use of memory, reasoning, and evaluation. Classification, or the organization of information, tends to be a major problem for children with IDD, as are memory problems, because children with IDD are less likely to rehearse information. • The issue of learned helplessness becomes a challenge for teachers of children with intellectual and developmental disabilities in inclusive settings because they are likely to see that their performance does not match that of the typical student and to avoid tasks that are difficult.
Children with IDD have a general deficit in language development and specific problems using interpretative language. The development of language in children who are IDD develops in the same fashion as it does in nondisabled individuals, only slower.. • We now know that emotional and social difficulties can create problems with vocational and community adjustment. Some skills can be attributed to positive social acceptance, such as taking turns, attending, following directions, and so forth. Social competence involves not only the presence of such skills but also the appropriate use of them in social situations
Educational Adaptations • Children with IDD often do not learn from observation or imitation and lack the strategies for attacking new or problem situations. Two of the special teaching strategies that are effective with children with IDD are scaffolding and reciprocal teaching. • Cooperative learning activities, problem-solving strategies, self-management strategies, and social skills training can help students with IDD become socially competent and confident. • Positive behavior supports Positive behavior supports (PBS) or Functional behavioral Analysis: An approach to intervention based on behavior science principles and meant to replace punitive measures for behavior control. It includes functional assessments, positive interventions, and evaluative measures to assess progress.
Modeling Introducing a skill through live audio or video demonstrations. • The rapidly developing technology can greatly assist students with IDD. Computers can be useful for drill and practice, tutorials, simulations, and problem solving.
Transition • The law requires that the IEP team begin no later than age 14 to address the student's need for instruction that will assist him or her in preparing for transition. • Beginning at age 16 (or younger, if determined appropriate by the IEP team), the IEP must contain a statement of needed transition services for the student, including, if appropriate, a statement of interagency responsibilities. This includes a coordinated set of activities with measurable outcomes that will move the student from school to post-school activities (work)
Regional Center: IPP’s ,Independent Living and Assisted living services • Department of Rehabilitation • Group Homes • In Home Supportive Services • Respite care