Download
1 / 17
170 likes | 347 Views
From Guidelines to Coverage . How are guidelines for health care policy to be reconciled with guidelines for clinical practice?. Louis B. Jacques, MD E-GAPPS Day 1, Theme I, Breakout 3. Challenges. Guidelines reflect wording to achieve consensus. May consider…alternative…YMMV*

E N D
From Guidelines to Coverage How are guidelines for health care policy to be reconciled with guidelines for clinical practice? Louis B. Jacques, MD E-GAPPS Day 1, Theme I, Breakout 3
Challenges • Guidelines reflect wording to achieve consensus. • May consider…alternative…YMMV* • Practitioners or interventions are not always clearly defined • Studied patient populations may not align with Medicare beneficiary population • Medicare regulations are interpreted with a precision not found in clinical guidelines. • You WILL or you WILL NOT… • Defined practitioner types • Content at the coding level of specificity • Real penalties • Elderly, permanently disabled, ESRD population YMMV: Your mileage may vary.
Outline • Medicare • Statute and regulation • NCD process • An Example (STIs) • Transparent development of guidelines and coverage policy • Historical record is available • Reflects recent practices
MIPPA (2008) SEC. 101. IMPROVEMENTS TO COVERAGE OF PREVENTIVE SERVICES. (a) Coverage of Additional Preventive Services- (1) COVERAGE- Section 1861 of the Social Security Act (42 U.S.C. 1395x), as amended by section 114 of the Medicare, Medicaid, and SCHIP Extension Act of 2007 (Public Law 110-173), is amended-- (A) in subsection (s)(2)-- (i) in subparagraph (Z), by striking ‘and’ after the semicolon at the end; (ii) in subparagraph (AA), by adding ‘and’ after the semicolon at the end; and (iii) by adding at the end the following new subparagraph: ‘(BB) additional preventive services (described in subsection (ddd)(1));’; and (B) by adding at the end the following new subsection:
More Statute Additional Preventive Services ‘(ddd)(1) The term ‘additional preventive services’ means services not described in subparagraph (A) or (C) of paragraph (3) that identify medical conditions or risk factors and that the Secretary determines are-- ‘(A) reasonable and necessary for the prevention or early detection of an illness or disability; ‘(B) recommended with a grade of A or B by the United States Preventive Services Task Force; and ‘(C) appropriate for individuals entitled to benefits under part A or enrolled under part B. ‘(2) In making determinations under paragraph (1) regarding the coverage of a new service, the Secretary shall use the process for making national coverage determinations (as defined in section 1869(f)(1)(B)) under this title. As part of the use of such process, the Secretary may conduct an assessment of the relation between predicted outcomes and the expenditures for such service and may take into account the results of such assessment in making such determination.’. (3) The term “preventive services” means the following: (A) The screening and preventive services described in subsection (ww)(2) (other than the services described in subparagraph (M) of such subsection). (B) An initial preventive physical examination (as defined in subsection (ww)). (C) Personalized prevention plan services (as defined in subsection (hhh)(1)). ***Note: highlighted language – modifications authorized by Section 4104 of the Affordable Care Act.
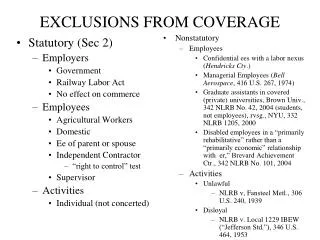
MEDICARE NATIONAL COVERAGE PROCESS* PreliminaryDiscussions Reconsideration 6 months or 9 months Benefit Category Final Decision Memorandum and Implementation Instructions Proposed Decision Memorandum Posted StaffReview National Coverage Request Public Comment External Technology Assessment Departmental Appeals Board Staff Review MEDCAC * SSA 1862(l)(1) –(l)(4) 6
42CFR 410.64 (a) Medicare Part B pays for additional preventive services not described in paragraph (1) or (3) of the definition of “preventive services” under §410.2, that identify medical conditions or risk factors for individuals if the Secretary determines through the national coverage determination process (as defined in section 1869(f)(1)(B) of the Act) that these services are all of the following: (1) reasonable and necessary for the prevention or early detection of illness or disability.(2) recommended with a grade of A or B by the United States Preventive Services Task Force, (3) appropriate for individuals entitled to benefits under Part A or enrolled under Part B. (b) In making determinations under paragraph (a) of this section regarding the coverage of a new preventive service, the Secretary may conduct an assessment of the relation between predicted outcomes and the expenditures for such services and may take into account the results of such an assessment in making such national coverage determinations. N.B. Emphasis added
USPSTF Created in 1984, the U.S. Preventive Services Task Force (USPSTF or Task Force) is an independent group of national experts in prevention and evidence-based medicine that works to improve the health of all Americans by making evidence-based recommendations about clinical preventive services such as screenings, counseling services, or preventive medications. The USPSTF is made up of 16 volunteer members who come from the fields of preventive medicine and primary care, including internal medicine, family medicine, pediatrics, behavioral health, obstetrics/gynecology, and nursing. All members volunteer their time to serve on the USPSTF, and most are practicing clinicians. N.B. Emphasis added
USPSTF and Primary Care The USPSTF conducts scientific evidence reviews of a broad range of clinical preventive health care services (such as screening, counseling, and preventive medications) and develops recommendations for primary care clinicians and health systems. The USPSTF strives to make accurate, up-to-date, and relevant recommendations about preventive services in primary care. Recommendations issued by the USPSTF are intended for use in the primary care setting. http://www.uspreventiveservicestaskforce.org/
National Coverage Analysis (NCA) for Screening for Sexually Transmitted Infections (STIs) and High-Intensity Behavioral Counseling (HIBC) to prevent STIs USPSTF A or B Recommendations • Screening for chlamydial infection for all sexually active non-pregnant young women aged 24 and younger and for older non-pregnant women who are at increased risk (A) • Screening for chlamydial infection for all pregnant women aged 24 and younger and for older pregnant women who are at increased risk (B) • Screening for gonorrhea infection in all sexually active women, including those who are pregnant, if they are at increased risk for infection (B) • Screening for syphilis infection for all pregnant women (A) and for persons at increased risk (A) • Screening for hepatitis B virus (HBV) infection in pregnant women at their first prenatal visit (A) • HIBC for the prevention of STIs for all sexually active adolescents, and for adults at increased risk for STIs (B) http://www.cms.gov/medicare-coverage-database/details/nca-details.aspx?NCAId=250&
Chlamydia and Gonorrhea • Pregnant women who are 24 years old or younger when the diagnosis of pregnancy is known, and then repeat screening during the third trimester if high-risk sexual behavior has occurred since the initial screening test. • Pregnant women who are at increased risk for STIs when the diagnosis of pregnancy is known, and then repeat screening during the third trimester if high-risk sexual behavior has occurred since the initial screening test. • Women at increased risk for STIs annually.
Syphilis • Pregnant women when the diagnosis of pregnancy is known, and then repeat screening during the third trimester and at delivery if high-risk sexual behavior has occurred since the previous screening test. • Men and women at increased risk for STIs annually.
Hepatitis B • Pregnant women at the first prenatal visit when the diagnosis of pregnancy is known, and then rescreening at time of delivery for those with new or continuing risk factors.
HIBC • In addition, effective for claims with dates of service on or after November 8, 2011, CMS will cover up to two individual 20- to 30-minute, face-to-face counseling sessions annually for Medicare beneficiaries for HIBC to prevent STIs, for all sexually active adolescents, and for adults at increased risk for STIs, if referred for this service by a primary care physician or practitioner, and provided by a Medicare eligible primary care provider in a primary care setting. Coverage of HIBC to prevent STIs is consistent with the USPSTF recommendation. • HIBC is defined as a program intended to promote sexual risk reduction or risk avoidance, which includes each of these broad topics, allowing flexibility for appropriate patient-focused elements: • education, • skills training, • guidance on how to change sexual behavior.
What is Primary Care for Medicare? • For the purposes of this NCD, a primary care setting is defined as the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care needs, developing a sustained partnership with patients, and practicing in the context of family and community. Emergency departments, inpatient hospital settings, ambulatory surgical centers, independent diagnostic testing facilities, skilled nursing facilities, inpatient rehabilitation facilities, clinics providing a limited focus of health care services, and hospice are examples of settings not considered primary care settings under this definition. • For the purposes of this NCD, a “ primary care physician” and “ primary care practitioner” will be defined based on existing sections of the Social Security Act (§1833(u)(6), §1833(x)(2)(A)(i)(I) and §1833(x)(2)(A)(i)(II)). • §1833(u) • (6) Physician Defined.—For purposes of this paragraph, the term “physician” means a physician described in section 1861(r)(1) and the term “primary care physician” means a physician who is identified in the available data as a general practitioner, family practice practitioner, general internist, or obstetrician or gynecologist. • §1833(x)(2)(A)(i)(I) is a physician (as described in section 1861(r)(1)) who has a primary specialty designation of family medicine, internal medicine, geriatric medicine, or pediatric medicine; or (II) is a nurse practitioner, clinical nurse specialist, or physician assistant (as those terms are defined in section 1861(aa)(5));
Implementation: Paying Claims A new HCPCS code, G0445, high-intensity behavioral counseling to prevent sexually transmitted infections, face-to-face, individual, includes: education, skills training, and guidance on how to change sexual behavior, performed semi-annually, 30 minutes, has been created for use when reporting HIBC to prevent STIs effective November 8, 2011, to be included in the January 2012 Medicare Physician Fee Schedule Database (MPFSDB) and Integrated Outpatient Code Editor (IOCE) updates. Code G0445 may be paid on the same date of service as an annual wellness visit, evaluation and management (E&M) code, or during the global billing period for obstetrical care, but only one G0445 may be paid on any one date of service. If billed on the same date of service with an E&M code, the E&M code should have a distinct diagnosis code other than the diagnosis code used to indicate high/increased risk for STIs for the G0445 service. An E&M code should not be billed when the sole reason for the visit is HIBC to prevent STIs. The appropriate screening diagnosis code (ICD-9 V74.5 – screening, bacterial – sexually transmitted, or V73.89 N.B. This is only 2 paragraphs from a 30 page set of contractor instructions. See the rest at: http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R2476CP.pdf
Ongoing Challenges • Subspecialists want to be classified as a primary care practitioners. • Non-physicians want to be recognized as physicians. • Facilities lacking bona fide primary care support infrastructure want to be classified as primary care practices. • Proprietary “sort of like” programs want to be recognized. • Coverage for FDA approved diagnostic tests versus “any” test. The debate continues…