Download
1 / 13
150 likes | 400 Views
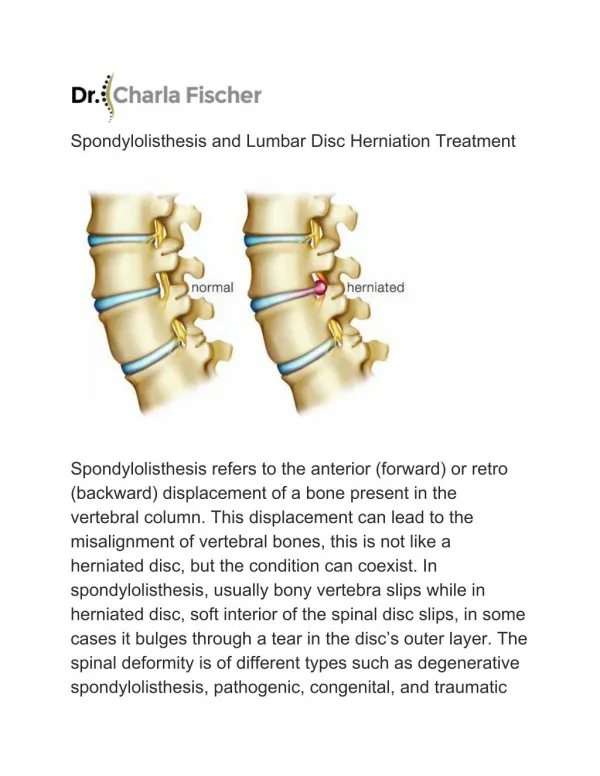
Alexandre A, Alexandre AM*, Paradiso R. XIX Symposium Neuroradiologicum The World Congress of Neuroradiology Bologna 2010, 4-9 October. Lumbar disc herniation treatment with microdiscectomy versus intradiscal oxygen-ozone injections. European Neurosurgical Institute (EU.N.I.). Treviso

E N D
Alexandre A, Alexandre AM*, Paradiso R XIX Symposium Neuroradiologicum The World Congress of Neuroradiology Bologna 2010, 4-9 October Lumbar disc herniation treatment with microdiscectomy versus intradiscal oxygen-ozone injections. European Neurosurgical Institute (EU.N.I.). Treviso *Institute of Radiology - Catholic University of Sacred Heart. Rome
Lumbar herniation level microdiscectomy discolysis L1-L2 1 (0,33%) 3 (1%) L2-L3 4 (1.33%) 3 (1%) L3-L4 28 (9.33%) 36 (12%) L4-L5 159 (53%) 165 (55%) L5-S1 108 (36%) 93 (31%) EU.N.I. www.eunionline.com
kind of herniation microdiscectomy discolysis • Contained 197 (65,6%) 200 (66.6%) • extruded 93 (31%) 82 (27,3%) • Migrated 10 (3,3%) 18 (6%) EU.N.I. www.eunionline.com
Pain Regression upon controls Controls Microdiscectomy Discolysis • 4-6 months 292 / 300 (97.3%) 280 (93,3%) • 1 year 275 (91,6%) 276 (92 %) • 3 years 250 (83,3%) 2 (87,3%) VAS Regression > 4 EU.N.I. www.eunionline.com
Pain Regression/ level,at 1 year Microdiscectomy Discolysis • L1-L2 1 (100%) 3 (100%) • L2-L3 3 (50%) 3 (100%) • L3-L4 24 (82.1%) 33 (91,6%) • L4-L5 143 / 159(89.9%) 150 / 165 (90.90%) • L5-S1 104 / 108 (96.2%) 88 / 93 (94.6%) VAS Regression > 4 EU.N.I. www.eunionline.com
Pain regression / kind • Hernia Microdiscectomy Discolysis • Contained 163/197 (82,74%) 172/200 (86%) • Extruded 85 / 93 (91,39%) 76 / 82 (92.6%) • Migrated 9 / 10 (90%) 15 / 18 (83.33%) Regression VAS > 4 EU.N.I. www.eunionline.com
Pain regression/Localisation Intraforaminal microdiscectomy discolysis • 22 (91,6%) 22 (84,6%) Regression VAS > 4 EU.N.I. www.eunionline.com
Sensory disfunction regression at 3 years Microdiscectomy Discolysis • complete 82.5 % 83.2 % • Partial 12.4 % 9.4 % • Insignificant 5.1% 2.4 % EU.N.I. www.eunionline.com
Motor Deficit regression at 3 years Microdiscectomy Discolysis • complete 86.6% 85.7% • partial 9.8 % 8.3% • Insignificant 3.6% 6 % EU.N.I. www.eunionline.com
Results • Complications observed in the two series of case records related to the procedure: • 4 fistulas of cerebrospinal fluid and 1 bacterial discitis in Microdiscectomy • 2 chemical discitis in Discolysis
Conclusion Results are overall better for percutaneous Discolysis in contained herniations, with broken annulus, under or extraligamentosus. On the other hand, results are totally better in cases of big extruded or migrated herniations, particular if pain was intolerable or there were important motor deficits.
Conclusion Microdiscectomy has a documented morbidity and mortality. A failure of Microdiscectomy is a FBSS (severe chronic postoperative pain, which is usually resistant to physiotherapy an pharmacological treatment). A Failure of Discolysis can't cause a FBSS, and rarely engenders new iatrogenic problems.
Conclusion Except than these considerations results are essentially equivalent with time considering both pain control and management of neurological deficits.