Download
1 / 56
560 likes | 809 Views
Staging Shakedown. Tonya Brandenburg, mha , ctr Nicole Catlett, Ctr. Colon and Rectum. EOD Primary Tumor Based on layer invasion and extension to adjacent organs/structures EOD Regional Nodes Based on regional nodes positive and location of LNs

E N D
Staging Shakedown Tonya Brandenburg, mha, ctr Nicole Catlett, Ctr
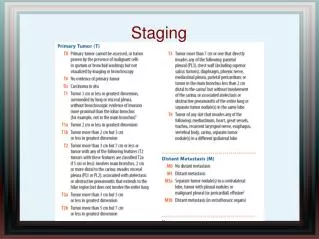
Colon and Rectum • EOD Primary Tumor • Based on layer invasion and extension to adjacent organs/structures • EOD Regional Nodes • Based on regional nodes positive and location of LNs • Regional nodes positive used with codes 300 & 800 for Derived EOD N • EOD Mets • Distant lymph nodes • Distant mets
Colon and Rectum - EOD Primary Tumor • Note 1: Code 000 (behavior code 2) includes cancer cells confined within the glandular basement membrane (intraepithelial), or described as in situ. • Note 2: Code 050 (behavior code 3) includes the following: • Intramucosal, NOS • Lamina propria • Mucosa, NOS • Confined to, but not through muscularis mucosa • Note 3: Ignore intraluminal extension to adjacent segment(s) of colon/rectum or to the ileum from the cecum; code depth of invasion or extracolonic spread as indicated.
Colon and Rectum- EOD Primary Tumor • Note 4: Tumor that is adherent to other organs or structures, macroscopically, is coded as 600 or 700. However, if no tumor is present in the adhesion, microscopically, the classification should be coded to 100-500. • Note 5: Tumors characterized by involvement of the serosal surface (visceral peritoneum) by direct extension or perforation in which the tumor cells are continuous with the serosal surface through inflammation are coded to 500.
Colon and Rectum - EOD Regional Nodes • Note 1: Code only regional nodes and nodes, NOS in this field. Distant nodes are coded in EOD Mets. • Note 2: For Colon and Rectum ONLY, any unnamed nodes that are removed with a colon or rectal resection are presumed to be regional pericolic or perirectal lymph nodes and are included in the EOD Regional Nodes code 300 (pericolic for sites C180 - C189, C199 and perirectal for sites C199 or C209).
Colon and Rectum - EOD Mets • Colon • Iliac (common, external) • Inferior mesenteric (cecum, ascending colon, hepatic flexure, transverse colon) • Para-aortic • Retroperitoneal • Superior mesenteric Note: Distant lymph node(s) for Colon, Rectum and Rectosigmoid include • Rectosigmoid/Rectum • Colic (left) (rectum) • Hemorrhoidal, inferior (rectosigmoid) • Iliac (common, external) • Internal iliac (hypogastric), NOS (rectosigmoid) • Obturator (rectosigmoid) • Rectal, inferior (rectosigmoid) • Superior mesenteric
Summary Stage 2018 Colon • Note 3: Code 0 (behavior code 2) includes cancer cells confined within the glandular basement membrane (intraepithelial), or described as in situ. • Note 4: For the following, AJCC 8th edition stages these as in situ tumors. SS2018 stages these as localized (behavior code 3) • Intramucosal, NOS • Lamina propria • Mucosa, NOS • Confined to, but not through muscularis mucosa • Note 5: Ignore intraluminal extension to adjacent segment(s) of colon/rectum or to the ileum from the cecum; code depth of invasion or extracolonic spread as indicated.
Summary Stage 2018 Colon • Note 6: Tumor that is adherent to other organs or structures, macroscopically, is coded as regional (code 2) or distant (code 7). However, if no tumor is present in the adhesion, microscopically, the classification should be coded to localized (code 1) or regional (code 2). • Note 7: Tumors characterized by involvement of the serosal surface (visceral peritoneum) by direct extension or perforation in which the tumor cells are continuous with the serosal surface through inflammation are coded to regional (code 2).
Prostate • EOD Primary Tumor • For Clinical Extension only • Based on lobe involvement, extension to adjacent organs/structures • Prostate Pathological Extension • For pathological assessment (prostatectomy) • Based on lobe involvement, extension to adjacent organs/structures EOD Regional Nodes • Based on location of LNs • EOD Mets • Distant lymph nodes • Bone involvement • Distant mets
Prostate - Additional Items for Staging • In addition to coding EOD Primary Tumor, EOD Regional Nodes and EOD Mets, the following data items are also needed to assign a stage group for Prostate. • PSA (Prostatic Specific Antigen) Lab Value • Grade Clinical • Grade Pathological
Prostate - EOD Primary Tumor • Note 1: This field and Prostate Pathological Extension, must both be coded, whether or not a prostatectomy was performed. Information from prostatectomy and autopsy is excluded from this field and coded only in Prostate Pathological Extension. • Note 2: Code 100 or 110 with a TURP only.
Prostate - EOD Primary Tumor • Note 3: Clinically inapparent and apparent tumor. When clinical apparency cannot be determined, code 300. • Clinically inapparent tumors are not palpable. Physician documentation of a DRE that does not mention a palpable "tumor", "mass", or "nodule" can be inferred as inapparent. • Imaging is not used to determine the clinical extension unless the physician clearly incorporates imaging findings into their evaluation. • Do not infer inapparent or apparent tumor based on the registrar's interpretation of other terms in the DRE or imaging reports. • Code 300 for localized cancer when it is unknown if the tumor is clinically apparent.
Prostate - EOD Primary Tumor • Note 4: This field is based on the DRE whether or not the tumor is clinically apparent or inapparent. Do not use biopsy results to code this field UNLESS they prove extraprostatic extension. • Note 5: If there is no information from the DRE, or the terminology used is not documented in Note 3, but the physician assigns a clinical extent of disease, the registrar can use that. • Example: DRE reveals prostate is “firm.” Physician stages the patient as a cT2a. • The T2a can be used since the physician has documented this. • Note 6: Involvement of the prostatic urethra does not alter the EOD code.
EOD Primary Tumor • Note 7: "Frozen pelvis" is a clinical term which means tumor extends to pelvic sidewall(s). In the absence of a more detailed statement of involvement, assign a description of frozen pelvis to code 700. • Note 8: When an incidental finding of prostate cancer is found during a prostatectomy for other reasons (for example, a cystoprostatectomy for bladder cancer), code 800 (no evidence of primary tumor) in this field. If there is no documentation regarding a normal prostate evaluation (physical examination or imaging) prior to prostatectomy/autopsy, code 999 (unknown; extension not stated) in this field.
Prostate Pathological Extension • Note 1: Only use histologic information from prostatectomy, including simple prostatectomy with negative margins, and autopsy in this field. Information from biopsy of extraprostatic sites is coded in EOD Primary Tumor. • Note 2: Code 900 if there is no prostatectomy performed within the first course of treatment. • Note 3: Limit information in this field to first course of treatment in the absence of disease progression.
Prostate Pathological Extension • Note 4: When prostate cancer is an incidental finding during a prostatectomy for other reasons (for example, a cystoprostatectomy for bladder cancer), use the appropriate code for the extent of disease found. • Note 5: Involvement of the prostatic urethra does not alter the extension code. • Note 6: "Frozen pelvis" is a clinical term which means tumor extends to pelvic sidewall(s). In the absence of a more detailed statement of involvement, assign this to code 700.
Prostate - EOD Regional Nodes • Note 1: Code only regional nodes and nodes, NOS, in this field. Distant nodes are coded in EOD Mets. • Note 2: Regional nodes include contralateral or bilateral nodes.
Prostate - EOD Mets • No extra notes just code as is!
PSA Lab Value • Note 1: Physician statement of prostatic specific antigen (PSA) pre-diagnosis can be used to code this data item when no other information is available. • Note 2: PSA is a prognostic factor required for AJCC staging. It affects the stage group in most cases. • Note 3: Record to the nearest tenth in nanograms/milliliter (ng/ml) the last pre-diagnosis PSA lab value prior to diagnostic biopsy of prostate and treatment. The lab value may be recorded in the lab report, history and physical, or clinical statement in the pathology report, etc. • A lab value expressed in micrograms per liter (ug/L) is equivalent to the same value expressed in nanograms per milliliter (ng/ml) • Record 0.1 when the lab results are stated as less than 0.1 ng/ml with no exact value. • For an uncertain value, record the stated closest value. For example, code a value stated as "less than 5.0 ng/ml" as 4.9. Examples: PSA of 7.2. Code 7.2 PSA of 8.56. Code 8.6 PSA of 10. Code 10.0 PSA of 110.35. Code 110.4
PSA Lab Value • Note 4: A discrepancy between the PSA documented in the lab report and the PSA documented by the clinician may arise due to the clinician’s adjusting the PSA value. Certain medications for benign prostatic hypertrophy (BPH) decrease the PSA. • If there is documentation by a clinician within the medical record of an adjusted PSA value, record the adjusted value. • The registrar does not adjust the PSA value based on BPH medication use. • If there is no documentation by a clinician within the medical record of an adjusted PSA value, record the PSA value provided. • The fact that an adjusted PSA value is being recorded should be documented in the Dx Proc – Lab Tests text field.
Prostate - Grade Clinical • Note 1: Clinical grade must not be blank. • Note 2: Assign the highest grade from the primary tumor assessed during the clinical time frame. • Note 3: Codes 1-5 take priority over A-E. • Note 4: Code 9 when • Grade from primary site is not documented • Clinical workup is not done (for example, cancer is an incidental finding during surgery for another condition) • Grade checked “not applicable” on CAP Protocol (if available) and no other grade information is available
Prostate - Grade Clinical • Note 5: If there is only one grade available and it cannot be determined if it is clinical, pathological, or after neo-adjuvant therapy, assign as a clinical grade and code unknown (9) for pathological grade, and blank for post-therapy grade. • Note 6: If you are assigning an AJCC 8th edition stage group • Grade is required to assign stage group • Codes A-E are treated as an unknown grade when assigning AJCC stage group • An unknown grade may result in an unknown stage group
Prostate - Grade Pathological • Note 1: Pathological grade must not be blank. • Note 2: Assign the highest grade from the primary tumor. If the clinical grade is higher than the grade determined during the pathological time frame, use the grade that was identified during the clinical time frame for both the clinical grade and the pathological grade. • Note 3: Codes 1-5 take priority over A-E.
Prostate - Grade Pathological • Note 4: Code 9 when • Grade from primary site is not documented • No resection of the primary site • Neo-adjuvant therapy is followed by a resection (see post-therapy grade) • Clinical case only (see clinical grade) • There is only one grade available and it cannot be determined if it is clinical, pathological, or after neo-adjuvant therapy • Grade checked “not applicable” on CAP Protocol (if available) and no other grade information is available • Note 5: If you are assigning an AJCC 8th edition stage group • Grade is required to assign stage group • Codes A-E are treated as an unknown grade when assigning AJCC stage group • An unknown grade may result in an unknown stage group
Summary Stage 2018 Prostate • Note 4: Assign code 1 when there is only a TURP. • Note 5: Imaging is not used to determine the clinical extension unless the physician clearly incorporates imaging findings into their evaluation. • Note 6: If there is no information from the DRE, but the physician assigns a clinical extent of disease, the registrar can use that. • Example: DRE reveals prostate is “firm.” Physician stages the patient as a cT2a. • The T2a (localized) can be used since the physician has documented this.
Summary Stage 2018 Prostate • Note 7: Involvement of prostatic urethra does not alter the Summary Stage code. • Note 8: “Frozen pelvis” is a clinical term which means tumor extends to pelvic sidewall(s) (code 7). • Note 9: When prostate cancer is an incidental finding during a prostatectomy for other reasons (for example, a cystoprostatectomy for bladder cancer), use the appropriate code for the extent of disease found.
Number of Cores Positive • Notes • Note 1: Physician statement of Number of Cores Positive can be used to code this data item when there is no other information available. • Note 2: Record the number of positive prostate core biopsies from the first prostate core biopsy diagnostic for cancer. If positive cores are identified and the number of positive cores not specifically documented, code X6. • Note 3: If the pathology report contains a summary of the number of cores positive and examined, use the summary provided. If Summary Report is not available and multiple biopsy cores are obtained on the same day, the number of cores examined should be added. • Note 4:Transperineal template-guided saturation biopsy (TTSB) is a stereotactic prostate biopsy technique that typically produces 30 to 80 core biopsies. This is an alternative biopsy technique used for some high-risk patients including men with persistently elevated PSA, those who have atypia on prior prostate biopsies, or men with biopsies showing high grade prostatic intraepithelial neoplasia (PIN). • Note 5: The number of cores examined are recorded in Number of Cores Examined [NAACCR Data Item # 3897].
Number of Cores Examined • Notes • Note 1: Physician statement of Number of Cores Examined can be used to code this data item when there is no other information available. • Note 2: Record the number of prostate core biopsies examined from the first prostate core biopsy diagnostic for cancer. If the number of cores examined is not specifically documented, code X6. • Note 3: If the pathology report contains a summary of the number of cores positive and examined, use the summary provided. If Summary Report is not available and multiple biopsy cores are obtained on the same day, the number of cores examined should be added. • Note 4:Transperineal template-guided saturation biopsy (TTSB) is a stereotactic prostate biopsy technique that typically produces 30 to 80 core biopsies. This is an alternative biopsy technique used for some high-risk patients including men with persistently elevated PSA, those who have atypia on prior prostate biopsies, or men with biopsies showing high grade prostatic intraepithelial neoplasia (PIN). • Note 5: The number of cores positive are recorded in Number of Cores Positive [NAACCR Data Item # 3898].
Colon Case Example #1 • A 50 yowm presents for his first screening colonoscopy where a polyp was found in the sigmoid colon. A polypectomy was performed and path revealed a tubulovillous adenoma with intramucosal carcinoma. Stalk margin was negative. CEA was not performed. CT abdomen & pelvis was negative. No other treatment provided. A repeat surveillance colonoscopy 3 months later showed no residual/recurrent polyp.
Colon Case Example #1Coding Topography/Histology • Topography = c18.7 Sigmoid (per c-scope/polypectomy) • Histology = 8140/3 Adenocarcinoma (coded to adenocarcinoma per Solid Tumor Rules, don’t code to the polyp). • *Behavior note: SEER considers intramucosal to be invasive while AJCC derives Tis. So, you must code your behavior to /3 invasive.
Colon Case Example #1Coding EOD/SS2018 • EOD Primary Tumor = 050 Intramucosal (per path). • If you have coded your behavior incorrectly as /2 then you will get an error in CPDMS when trying to use this EOD T code. You will then need to key change your case to behavior /3 in order to code correctly. EOD Regional Nodes = 000 No involvement of regional LNs (per CT and also non-invasive). EOD METS = 000 No distant METS (per CT and also non-invasive). SS2018 = Localized, code 1 • Remember SEER considers invasive so you will get an error in CPDMS if you code 0 in-situ/non-invasive).
Colon Case Example #1Coding SSDIs • Grade Clinical = 9 unknown (not applicable as diagnosed at time of definitive surgery). • Grade Pathological = 9 unknown (not mentioned on path). • Grade Post-Therapy = blank (no preop/neoadjuvant TX given). • CEA pre-TX value = XXXX.9 CEA not done/unknown (no code for test not done) • CEA pre-TX interpretation = 9 unknown (not done). • Tumor Deposits = X9 No surgical resection performed (only polypectomy performed). • Perineural Invasion = 9 Not mentioned on path report. • Circumferential Resection Margin = XX.7 No surgical resection performed (only polypectomy). • KRAS = 9 unknown (not mentioned, no code for test not done). • MSI = 9 unknown (not mentioned, no code for test not done).
Colon Case Example #2 • A 67 yowf presents with abdominal pain and rectal bleeding. CT A/P was performed which revealed a tumor in the cecum extending through the bowel wall w/ adjacent LAD suspicious for METS. Multiple liver nodules compatible w/ METS. CT chest showed no evidence of disease. Preop CEA was 10 and stated to be elevated. PT was taken to surgery for exploratory LAP and R hemicolectomy was performed. Surgeon mentions in OP that tumor was identified in the cecum. Path: Mucinous Adenocarcinoma, poorly differentiated, 4 cm in size, invading through the serosa into the abdominal wall, PNI identified, margins negative, distance from CRM 2 cm, 3 tumor deposits, 13/13 regional LNs were positive. Tru-Cut liver BX was also positive for METS. FOLFOX initiated shortly after surgery.
Colon Case Example #2Coding Topography/Histology • Topography = c18.0 Cecum (per OP report). • Histology = 8480/3 Mucinous Adenocarcinoma per path.
Colon Case Example #2Coding EOD/SS2018 • EOD Primary Tumor = 600 Invasion of abdominal wall per path. • EOD Regional Nodes = 300 Involvement of pericolic LNs per path & • Note 2 above schema. • EOD METS = 20 Distant METS to single organ – Liver per path & imaging. • SS2018 = Distant, code 7
Colon Case Example #2Coding SSDIs • Grade Clinical = 9 unknown (not applicable as no BX was performed prior to resection). • Grade Pathological = 3 poorly differentiated per path (colon now coded using 4-tier system). • Grade Post-Therapy = blank (no preop/neoadjuvant TX given). • CEA pre-TX value = 10.0 preTX CEA 10.0 ng/mL. • CEA pre-TX interpretation = 1 preTX CEA stated to be elevated by MD. • Tumor Deposits = 03 TDs identified: 3 per path. • Perineural Invasion = 1 PNI identified per path. • Circumferential Resection Margin = 20.0 CRM 2.0 cm per path. • KRAS = 9 unknown (not mentioned, no code for test not done). • MSI= 9 unknown (not mentioned, no code for test not done).
Colon Case Example #3 • A 48 yo Asian female presents with rectal bleeding. A screening colonoscopy revealed a transverse colon mass which BX path showed invasive adenocarcinoma, moderately differentiated. CT A/P showed no evidence of METS. Preop CEA was stated to be normal but actual value not stated. A segmental resection was performed with surgeon palpating the tumor in the mid transverse colon, Path showed adenocarcinoma, moderately differentiated, invading pericolic fat, negative margins, CRM 3 mm, no TDs, PNI not present, 20 benign LNs.
Colon Case Example #3Coding Topography/Histology • Topography = c18.4 Transverse (per OP report). • Histology = 8140/3 Adenocarcinoma per path.
Colon Case Example #3Coding EOD/SS2018 • EOD Primary Tumor = 400 Invasion of pericolic fat per path. • EOD Regional Nodes = 000 No involvement of regional LNs per path. • EOD METS = 00 No distant METS per imaging. • SS2018 = Regional extension, code 2 (pericolic fat).
Colon Case Example #3Coding SSDIs • Grade Clinical = 2 moderately differentiated per BX path. • Grade Pathological = 2 moderately differentiated per path (colon now coded using 4-tier system). • Grade Post-Therapy = blank (no preop/neoadjuvant TX given). • CEA pre-TX value = XXXX.7 preTX CEA ordered, results not on chart/unknown. • CEA pre-TX interpretation = 0preTX CEA stated to be normal by MD. • Tumor Deposits = 00 No TDs identified per path. • Perineural Invasion = 0 PNI not identified per path. • Circumferential Resection Margin = 03.0 CRM 3.0 mm per path. • KRAS = 9 unknown (not mentioned, no code for test not done). • MSI= 9 unknown (not mentioned, no code for test not done).
Prostate Case Example #1 • A 64 yowm presents with an elevated PSA of 4.1 and abnormal DRE with a small nodule present in R mid gland. TRUS w/ BX revealed Adenocarcinoma, gleason 6 (3+3), grade group 1, present in 3 cores out of 12 examined. The positive cores were from the R side. CT A/P & bone scan were performed and showed no evidence of METS. Patient followed back w/ urologist, where he chose active surveillance for cT2aN0M0 Stage I prostate cancer.
Prostate Example #1Coding Topography/Histology • Topography = c61.9 Prostate • Histology = 8140/3 Adenocarcinoma per path.
Prostate Example #1Coding EOD/SS2018 • EOD Primary Tumor = 200 Clinically apparent tumor involving one-half of one side or less per DRE & MD staging. • Pathologic Extension = 900 No prostatectomy performed • EOD Regional Nodes = 000 No involvement of regional LNs per CT. • EOD METS = 00 No distant METS per imaging. • SS2018 = Localized, code 1.
Prostate Case Example #1Coding SSDIs • Grade Clinical = 1 Grade group 1: Gleason 6 per BX path. • Grade Pathological = 9 not applicable (no surgery performed). • Grade Post-Therapy = blank (no preop/neoadjuvant TX given). • PSA lab value = 4.2 PSA 4.2 per H&P. • Number of cores positive = 03 per path. • Number of cores examined = 12 per path. • Gleason score clinical = 06 Gleason 6 per path. • Gleason pattern clinical = 33 Gleason 3+3 path. • Gleason score pathological = X7 No prostatectomy performed. • Gleason patterns pathological = X7 No prostatectomy performed. • Gleason tertiary pattern = X7 No prostatectomy performed.
Prostate Case Example #2 • A 81 yowm presents to ER w/ complaints of severe R hip pain.CT imaging performed showed an enlarged & abnormal prostate w/ bil external iliac LNs suspicious for prostatic malignancy w/ regional nodal involvement. Also noted was osseous METS in R iliac bone. CT chest was negative. PSA was elevated at 88.5 and DRE revealed invasion of the rectal wall. PT opted for Hospice care.
Prostate Example #2Coding Topography/Histology • Topography = c61.9 Prostate • Histology = 8140/3 Adenocarcinoma per path.
Prostate Example #2Coding EOD/SS2018 • EOD Primary Tumor = 600 Invasion of rectum per DRE. • Pathologic Extension = 900 No prostatectomy performed. • EOD Regional Nodes = 300 Involvement of bil external iliac LNs per CT. • EOD METS = 30 Bone METS w/out distant LNs per imaging. • SS2018 = Distant, code 7.
Prostate Case Example #2Coding SSDIs • Grade Clinical = 9 Grade unk/no BX of prostate performed. • Grade Pathological = 9 not applicable (no surgery performed). • Grade Post-Therapy = blank (no preop/neoadjuvant TX given). • PSA lab value = 88.5 PSA 88.5 per H&P. • Number of cores positive = X7 no needle core BX performed. • Number of cores examined = X7 no needle core BX performed. • Gleason score clinical = X7 no needle core BX/TURP performed. • Gleason pattern clinical = X7 no needle core BX/TURP performed. • Gleason score pathological = X7 No prostatectomy performed. • Gleason patterns pathological = X7 No prostatectomy performed. • Gleason tertiary pattern = X7 No prostatectomy performed.
Prostate Case Example #3 • A 52 yo black male with HX of BPH who comes in for a TURP. • TURP performed with path showing Gleason 7 (3+4) Adenocarcinoma in 2% of tissue resected. • CT A/P performed showed no evidence of disease. • PSA was stated to be normal, but value not on chart or mentioned in H&P • PT strongly wanted a prostatectomy due to +FHX in father. Radical prostatectomy performed showing Acinar Adenocarcinoma, Gleason (3+3), multiple microscopic foci present confined to the prostate, pT2, no LVI, No extraprostatic extension present, margins negative, & no LNs received for exam.