Download
1 / 1
10 likes | 141 Views
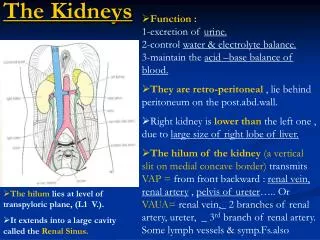
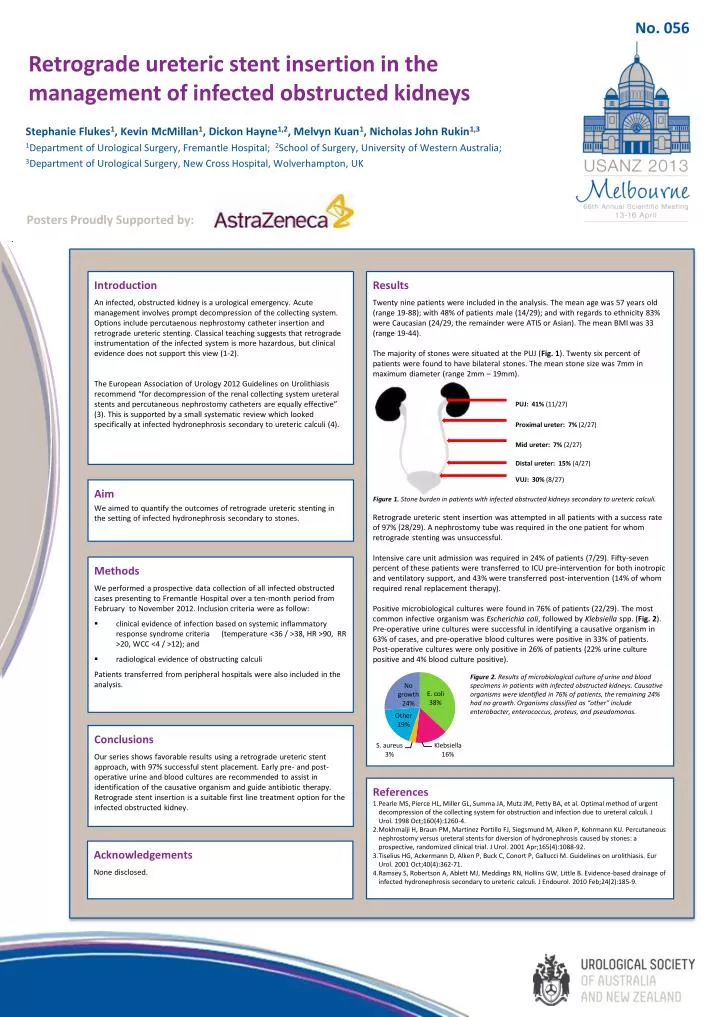
No. 056. Retrograde ureteric stent insertion in the management of infected obstructed kidneys. Stephanie Flukes 1 , Kevin McMillan 1 , Dickon Hayne 1,2 , Melvyn Kuan 1 , Nicholas John Rukin 1,3

E N D
No. 056 Retrograde ureteric stent insertion in the management of infected obstructed kidneys Stephanie Flukes1, Kevin McMillan1, Dickon Hayne1,2, Melvyn Kuan1, Nicholas John Rukin1,3 1Department of Urological Surgery, Fremantle Hospital; 2School of Surgery, University of Western Australia; 3Department of Urological Surgery, New Cross Hospital, Wolverhampton, UK Posters Proudly Supported by: PUJ: 41% (11/27) Introduction An infected, obstructed kidney is a urological emergency. Acute management involves prompt decompression of the collecting system. Options include percutaenous nephrostomy catheter insertion and retrograde uretericstenting. Classical teaching suggests that retrograde instrumentation of the infected system is more hazardous, but clinical evidence does not support this view (1-2). The European Association of Urology 2012 Guidelines on Urolithiasis recommend “for decompression of the renal collecting system ureteral stents and percutaneous nephrostomy catheters are equally effective” (3). This is supported by a small systematic review which looked specifically at infected hydronephrosis secondary to ureteric calculi (4). Results Twenty nine patients were included in the analysis. The mean age was 57 years old (range 19-88); with 48% of patients male (14/29); and with regards to ethnicity 83% were Caucasian (24/29, the remainder were ATIS or Asian). The mean BMI was 33 (range 19-44). The majority of stones were situated at the PUJ (Fig. 1). Twenty six percent of patients were found to have bilateral stones. The mean stone size was 7mm in maximum diameter (range 2mm – 19mm). Retrograde ureteric stent insertion was attempted in all patients with a success rate of 97% (28/29). A nephrostomy tube was required in the one patient for whom retrograde stenting was unsuccessful. Intensive care unit admission was required in 24% of patients (7/29). Fifty-seven percent of these patients were transferred to ICU pre-intervention for both inotropic and ventilatory support, and 43% were transferred post-intervention (14% of whom required renal replacement therapy). Positive microbiological cultures were found in 76% of patients (22/29). The most common infective organism was Escherichia coli, followed by Klebsiella spp. (Fig. 2). Pre-operative urine cultures were successful in identifying a causative organism in 63% of cases, and pre-operative blood cultures were positive in 33% of patients. Post-operative cultures were only positive in 26% of patients (22% urine culture positive and 4% blood culture positive). Proximal ureter: 7% (2/27) Mid ureter: 7% (2/27) Distal ureter: 15% (4/27) Aim We aimed to quantify the outcomes of retrograde ureteric stenting in the setting of infected hydronephrosissecondary to stones. Figure 1. Stone burden in patients with infected obstructed kidneys secondary to ureteric calculi. VUJ: 30% (8/27) • Methods • We performed a prospective data collection of all infected obstructed cases presenting to Fremantle Hospital over a ten-month period from February to November 2012. Inclusion criteria were as follow: • clinical evidence of infection based on systemic inflammatory response syndrome criteria (temperature <36 / >38, HR >90, RR >20, WCC <4 / >12); and • radiological evidence of obstructing calculi • Patients transferred from peripheral hospitals were also included in the analysis. Figure 2. Results of microbiological culture of urine and blood specimens in patients with infected obstructed kidneys. Causative organisms were identified in 76% of patients, the remaining 24% had no growth. Organisms classified as “other” include enterobacter, enterococcus, proteus, and pseudomonas. Conclusions Our series shows favorable results using a retrograde ureteric stent approach, with 97% successful stent placement. Early pre- and post-operative urine and blood cultures are recommended to assist in identification of the causative organism and guide antibiotic therapy. Retrograde stent insertion is a suitable first line treatment option for the infected obstructed kidney. References Pearle MS, Pierce HL, Miller GL, Summa JA, Mutz JM, Petty BA, et al. Optimal method of urgent decompression of the collecting system for obstruction and infection due to ureteral calculi. J Urol. 1998 Oct;160(4):1260-4. Mokhmalji H, Braun PM, Martinez Portillo FJ, Siegsmund M, Alken P, Kohrmann KU. Percutaneous nephrostomy versus ureteral stents for diversion of hydronephrosis caused by stones: a prospective, randomized clinical trial. J Urol. 2001 Apr;165(4):1088-92. Tiselius HG, Ackermann D, Alken P, Buck C, Conort P, Gallucci M. Guidelines on urolithiasis. Eur Urol. 2001 Oct;40(4):362-71. Ramsey S, Robertson A, Ablett MJ, Meddings RN, Hollins GW, Little B. Evidence-based drainage of infected hydronephrosis secondary to ureteric calculi. J Endourol. 2010 Feb;24(2):185-9. Acknowledgements None disclosed.