Download
1 / 17
250 likes | 843 Views
Hepatitis D . DR SACHIN VERMa MD( Medicine), ficm,fccs Consultant internal medicine & critical care Ivy hospital mohali. Introduction. Recognized in 1977 – co existent with HBV infection A defective RNA virus than need hepadnavirus (HBV) to replicate

E N D
Hepatitis D DR SACHIN VERMa MD( Medicine),ficm,fccs Consultant internal medicine & critical care Ivy hospital mohali
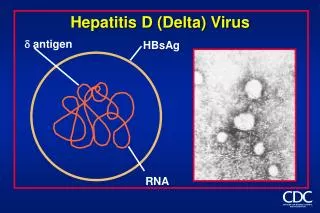
Introduction Recognized in 1977 – co existent with HBV infection A defective RNA virus than need hepadnavirus (HBV) to replicate 1980 – noticed the dependency of HDV to HBV (need HBsAg to as virion coat) Associated with most severe form of acute and chronic HBsAg +
Epidemiology of Hepatitis D • Spread worldwide • Highest in Russia, Romania, Southern Italy, Mediterranean countries, Africa, South America • Low in China, Taiwan, India • Latest trends • New foci in Okinawa, certain area of China, India, Albania • Decreasing trend in Mediterranean
Prevalence in region New Delhi : 8.1% in 1996[Irshad M et al. Eur J GastroenterolHepatol 1996; 8: 995-99816] New Delhi: 10.6% in 2005[Chakraborty P et al. Indian J Med Res2005; 122: 254-25715] Chandigarh :14.2%[Singh et al. J Viral Hepat1995; 2: 151-15417]. Ludhiana:10% in HBsAg-positive patients[Ghuman et al. Indian J Med Sci 1995; 49: 227-23023].
Mode of Transmission • Spread • Percutaneous and sexually and through body fluid/blood • Potentially infectious in whole phase • People at risk • HBV carrier, HBV unvaccinated person • IVDU • Unprotected sex • Exposed to unscreen blood, body fluid • People receiving blood, blood product
Hepatitis D Features IP – 5 to 64 days Super-infection* or co-infection with HBV
CLINICAL FEATURES : In acute CO-Infection • jaundice ,fatigue, abdominal pain, loss of appetite , nausea, vomiting ,joint pain, dark (tea colored) urine • In super-infection CLD and HCC.
DIAGNOSIS Following HBV-HDV co-infection both IgM anti-HDV during the acute illness and IgG anti-HDV during convalescence are detectable Following HBV-HDV super infection, chronic HDV infection with detectable HDAg usually occurs. Both IgM anti-HDV and IgG anti-HDV remain detectable.
DIAGNOSIS Anti LKM3 antibodies
Prevention • HBV-HDV Coinfection Pre or postexposure prophylaxis to prevent HBV infection. • HBV-HDV Superinfection Education to reduce risk behaviors among persons with chronic HBV infection
TREATMENT: • Acute HDV infection • Supportive care • Chronic HDV infection • interferon-alfa • liver transplant
a-interferon 2b 9 mu sc tiw, Rx > 12 months • 21-50% lose HDV RNA and have improved histology • Relapse occurs in almost all patients stopping treatment • Can stop treatment if HBV Surface Ag disappears (rare)