Download
1 / 22
220 likes | 227 Views
Vascular Analysis of Disease. In Nuclear Medicine. Blood Flow to the Extremities. Consider chronic or acute disease Blood flow interruption from arterial occlusions Embolism, thrombus, or a vascular injury

E N D
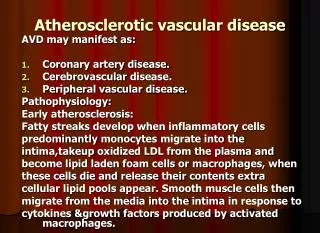
Vascular Analysis of Disease In Nuclear Medicine
Blood Flow to the Extremities • Consider chronic or acute disease • Blood flow interruption from arterial occlusions • Embolism, thrombus, or a vascular injury • Most procedures analyze venous blood flow and physiological uptake of the radiotracer • However, given certain situations arterial evaluation should be considered
Clinically Speaking • Regional distribution of vascular flow can be done using stress and rest procedures – Sound familiar? • Graft patency via blood flow determine viability • Evaluation of: ischemic ulcers and pre-amputation • AV malformation, shunts, vascular tumors, embolization • Venous evaluation of infection and DVTs • Angiography issue is its failure to evaluate collateral circulation • Is there collateral circulation that contrast files to image • Post injection contrast does not evaluate physiology
Xenon Utilization Purpose – To evaluate blood flow in muscle tissue • Think of 133Xe and its imaging characteristics • 0.1 mL saline with 100 μCi 133Xe injected IM 1 to 2 cm into muscle • Needle is not removed for 30 seconds, but images or data is collected in a serial mode • Declining activity is quantified with semilog paper • Procedure is done twice: stress and rest Lower extremities • Normal - 2 (rest) and 50 (stress) mL/min/100g • Abnormal - <20 (stress) mL/min/100g
Arterial Evaluation • Siegel el al. injected 99mTcHAM into the descending aorta or femoral artery • Rest and stress images taken in the extremities • Compared with contrast angiography • Disease was confirmed in both: large vessel occlusion, small vessel disease, ischemic ulcers, and other • Test is rarely done with arterial injection because of its invasive nature
Diffusible Tracer • While a patient underwent 201Tl in cardiology whole body scans were performed to evaluate muscle distribution of the tracer • Segall et al. noted stress and redistribution images in the legs with peripheral vascular disease • Normal patients: Leg activity = 25% of the total dose with stress having a greater amount than rest • Abnormal – Rest imaging in the leg had higher levels of activity when compared with stress indicating disease
Types of Vascular Evaluation • Determining the level or area of amputation based on ischemic areas in an extremity • mL/min/100g evaluated at three points using 133Xe: above the knee, below the knee, and the foot • Evaluate the pedicle flaps in reconstructive surgery • mL/min/100g used with 133Xe and 99mTcO4- • If a probe recorded delayed clearance, graft was not viable • Determine treatment of skin ulcers • Similar - mL/min/100g analysis used
Frost Bite and Electrical Burns Frost Bite • 99mTcO4- used to evaluate viable from non-viable tissue in the finger and toes. Lack of activity indicated loss of blood flow Electrical Burns • Using 99mTcPYP extent of muscle damage can be determined • Lacking uptake and flow was an indication of necrotic tissue • Delayed images also showed a donut shapes (cold center) and focal hotspots indicating damaged viable to the tissue
Monitoring Therapeutic Embolization • Polyvinyl alcohol spongelike (Ivalon) particles are used to occlude AV malformation and vascular tumors • Particles are tagged with 99mTcsulfur colloid so that the procedure can be monitored for its effectiveness • Catheter inserted and placed at the site of interest where embolization occurs • If too Ivalon particles appear in the lung “PE” type issues occur, requiring catheter adjustment
Repair of an Aneurysm • 99mTcRBCs are injected IV to identify an aneurysm. • Green arrows indicate aneurysm • Purple indicate repair • Note the difference in radiopharmaceutical distribution
Diagnosis of DVTs • Contrast venography (gold standard) – 100 mL contrast injected into the dorsal vein in the foot • DVT is diagnosed when flow abruptly stops or lack of deep vein filling occurs • Impedance Plethysmography (IPG) – Using an inflated thigh cuff, blood flow impedance is measure • Releasing cuff pressure and the lack reduced venous pressure via its electrical impedance is an indication of DTV
Diagnosing DVT (cont.) Ultrasound • Color Doppler with compression technique is used to detect DVT • Color separates venous (blue) from arterial (red) • Compression without the vein compressing indicates DVT
DVT/NMT Procedure • Most common radiopharmaceutical is 99mTcMAA where bilateral IV is setup, one for each foot • 1 – 2 mCi are injected at the same time with serial imaging • Alternative approach – tourniquet is applied at different points on the leg and a set of injections with serial images are taken • Detector placement must done at different intervals • Tib/fib, knees, and thigh • Depends on the size of the detector
Biodistribution of the Particles • Electrostatic forces between MAA and DVT cause the particles to stick to the DVT • Perfusion lung can now follow this procedure • What happens when you flush your syringe when injecting for a perfusion lung scan?
AcuTect: General Information • Used to diagnosis DVT • A synthetic peptide (not a MoAb!) - Apcitide • Binds to glycoprotein GP IIb/IIIa • platelet receive signals that cause activation and aggregation of the thrombus • Aggregation depended on GP IIb/IIIa receptor • AcutTect binds adhesion-molecule receptors found in the accute DVT • Was quickly approved by the FDA • Produced by Diatide, Incorporated and distributed by Nycomed Amersham
AcuTect: Clinical Trails(General) • Two clinical trials where completed on patients suspected of having DVT • Study A = 136 patients • Study B = 145 patients • All patients where analyzed with AcutTect and Contrast Venography • Total of 236 patients where finally processed
AcuTect: Clinical Trails - NMT Results • Independently evaluated by NM physicians • Data collected at 10, 60,.120, 180 minutes • Asymmetry on early and delays defined a DVT
AcuTect: Clinical Trails Contrast Venography • Two groups of radiologies evaluated the data • Group 1: Three independent radiologists from the imaging centers • Blinded to all other clinical data • No established reading criteria defined • Group 2: Three radiologists at one research center • Blinded to all other clinical data • Established criteria
AcuTect: Clinical Trails Results • AcuTect Results • Study A = 54 (48%) • Study B = 41 (33%) • Contrast Venography Results from Group 1 • Study A = 51 (45%) • Study B = 101 (82%) • Contrast Venography Results from Group 2 • Study A = 24 (21%) • Study B = 40 (33%) • AcuTect vs Group 2 (Research Center) Agreement rate • Study A = 56-71% • Study B = 66-73%
AcuTect: Comments/ Recommendations • Literature research seems limited • Can it be done before or after a V/Q lung scan? • Protocol suggest 10 and 60 minute delayed images • Digital image for contrast enhancement • Small peptides may be immunogenic • 642 observed for 3 hours • 1 patient became hypotensive from 10 to 60 minutes post dose
AcuTech: Normal variants • Collateral and superficial veins • Postsurgical sites • Nonvascular locations: joints, prostheses, muscle, skin, and soft tissue • Key - If the uptake does not persist in the late images then its normal
AcuTech Case Study • 29 year old male hospitalized with extensive burns presented with a 2 day history of left calf and knee pain. The suspected area was warm to the touch. • Increased persistent uptake is noted in the distal femoral, popliteal, and posterior calf vein. • Confirmed with contrast venography