Download
1 / 15
150 likes | 217 Views
4 Steps to Providing Care to Transgendered Patients. Pacific AIDS Education and Training Center Training for Trainers March, 2003 Curriculum developed by Samuel Lurie www.tgtrain.org. Welcome!. Training Goal.

E N D
4 Steps to Providing Care to Transgendered Patients Pacific AIDS Education and Training Center Training for Trainers March, 2003 Curriculum developed by Samuel Lurie www.tgtrain.org Welcome!
Training Goal • To examine specific health care and HIV prevention and treatment needs of transgendered people and to build skills for clinical providers to work more effectively with Transgendered people.
Learning Objectives At the end of the presentation, providers in attendance will: • 1) Understand basic definitions and range of transgender expressions, including differences in desire for and access to surgical or hormonal intervention. • 2) Distinguish between biological sex, gender identity and sexual orientation and ways in which care for transgendered populations specifically differs from care for Gay, Lesbian and Bisexual communities. • 3) Become familiar with protocols for care for Transgendered people and examine methods for collaboration and referral with other providers with expertise in working with transgendered people. • 4) Identify 2-3 barriers within their agencies or practice and solutions to those barriers, including using principles of cultural competence to provide access to care for transgendered patients.
Training Study Findings 2001-2002 Needs Assessment of Health Care Providers showed:Face-to-face key informant interviews with providers around New England, funded with support of New England AIDS Education and Training Center • Experience with a range of transgendered expressions but lack of information on populations, terminology, differences • Desire to treat TG patients respectfully but admitted discomfort and lack of tools for specific interviewing/assessments. • Concern and frustration with lack of information, studies and research • Concern and frustration with lack of treatment guidelines, referral contacts and ways to advocate for transgender clients. • Time constraints create an overarching barrier in building trusting relationships with clients, and trusting relationships are integral to quality care
Four Steps to Providing Care • Understand range of gender expressions and differences in desire for and access to surgical or hormonal interventions. • Recognize distinctionsbetween gender identity and sexual orientation and understand differences (and similarities) in health care delivery needs. • Become familiar with local expertise, protocols, and access to collaboration and referral. • Establish policiesto make agencies more trans-friendly
Step 1: Recognize Range of Expressions and Desires • Many words to identify gender-variance, including: MTF, FTM, transman, transwoman, bi-gendered, gender-blender, phallic woman, passing man, she-male, femme queen, non-op, boi, two-spirit, new man, new woman, etc. • Identities can and do change, based on context, culture, geography, and individual’s place on their life journey • Hormones and surgical interventions may be desired in an order or degree other than what protocols dictate. • Watch for pathologizing/medicalizing situation (even words like “pre-op” and “post-op” assume “op” as final outcome. Also, emphasis is on genitals, not person.)
Step 2-Gender identity and sexual orientation are different things • Every individual has a biological sex, a gender identity and a sexual orientation. • All can be considered fluid. • Homophobia is different than Transphobia Being transgendered does not mean you’re gay and being gay does not mean you’re transgendered. • There is overlap, in part because gender variance is often seen in gay context. • Masculine females and feminine males are assumedto be gay; • “anti-gay” discrimination and violence often targets gender expression, not sexuality • Anatomy does not determine sexual orientation
Step 2, Distinctions continued • Coming out as gay is different than coming out as trans • Trans people are often outcast in G/L context. • How do we apply cultural competency lessons that apply around heterosexism to gender variance? • CDC categorizes MTFs and partners as MSM; neither partner self-identifies as MSM • Power relationship between provider and client is intensified; provider as gate-keeper who must give ongoing “approval” • TG people have particular relationship to medical technology, and need to access services through trans-identity
Step 3 –Finding protocols and expertise • Not enough providers doing this work. • Long waiting lists, inundated when known • Benjamin Standards of Care • Tom Waddell Clinic Protocols for Care • Real-world issues • Insurance and money • Informed Consent • Harm Reduction, or “low-threshold” services • Lack of long-term studies • Need for research, Trans issue is ‘hot’, how to do research while respecting choices
HIV Prevalence and Risks • Not many studies, but all show painfully high rates of HIV infection. • 35% in SF MTFs; 63% African-American MTFs (Clements-Nolle, Am. Journal of Public Health, June 2001) • 68% of MTF sex workers in Atlanta(Elifson et al, Am. Journal of Public Health, 1993) • Often people don’t know they are infected, or have no access to care. • In SF study, 50% of those who knew status, not receiving care. • CDC places TG people in MSM category for funding and prevention programs
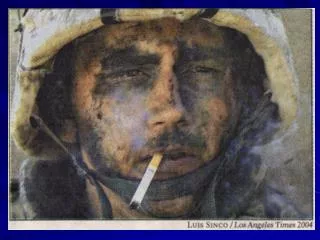
Medical-Related Trans Losses Billy Tipton Did not seek care for bleeding ulcer for fear of trans status being revealed. “Outed” in mass media upon his death. Tyra Hunter Died after paramedics withdrew treatment at scene of car accident. Robert Eads Died of ovarian cancer; refused treatment by a number of GYNs; difficult for FTMs to seek/receive GYN care. Alexander John Goodrum Trans activist and writer, died in a psychiatric facility. Photo by Mariette Pathy Allen Photos from Remembering Our Dead, www.gender.org/remember And Transsexual, Transgender and Intersexed History, www.transhistory.org
Step 4- Agency-related issues to provide services • Don’t just add “T” without doing work to understand what it means • Train all staff--receptionists, security guards, director • Make in-take forms trans friendly, i.e. include “chosen name” not just legal name; include more than M/F • Don’t make assumptions about sexuality or transition goals • Respect confidentiality, choices and fluidity • Honor presenting gender • Acknowledge limitations • Challenge transphobia—in staff and community • Have consequences for repeated anti-trans behavior • Have Unisex bathrooms!
Closing thought… “Working with someone going through a gender transition is a joyous part of medicine. It’s very similar to feelings obstetricians have about facilitating birth.” -Edward Cheslow, MD
Resources • Protocols for Hormonal Reassignment of Gender from the Tom Waddell Health Center, 2001,www.dph.sf.ca.us/chn/HlthCtrs/HlthCtrDocs/TransGendprotocols.pdf • Harry Benjamin International Gender Dysphoria Association (February 20, 2001). Standards of Care for Gender Identity Disorders, Sixth Version. www.hbigda.org/socv6.html • Oriel, K. A. (2000). Medical care of transsexual patients. Journal of the Gay and Lesbian Medical Association 4(4): 185-193 • AIDS Education and Training Centers National Resource Center: www.aidsetc.org, includes slides sets, links and other resources • Post, P, (2002), Crossing to Safety: Transgender Health and Homelessness, Healing Hands: A publication of the Health Care for the Homeless Clinician’s Network, 6 (4), June 2002. www.nhchc.org/Network/HealingHands/2002/June2002HealingHands.pdf • Bockting, W and Kirk S, editors, Transgender and HIV: Risks, prevention and care. Bringhamton, NY: The Haworth Press (2001) Originally published as a special issue of International Journal of Trangenderism 3.1+2. Available online at http://www.symposion/ijt
Resources continued • Clements-Nolle, K., Marx, R., Guzman, R., & Katz, M. (2001, June). “HIV prevalence, risk behaviors, health care use, and mental health status of transgender persons: implications for public health intervention.”American Journal of Public Health, 91(6), 915-921. • Keatley, J and Clements-Nolle, K. Factsheet: What are the Prevention Needs of Male-to-Female Transgender Persons? University of California, San Francisco, Center for AIDS Prevention Studies, (2001) (English and Spanish versions) www.caps.ucsf.edu • Gender Identity 101: A Transgender Primerby Alexander John Goodrum, a publication of TGNet Arizona, www.tgnetarizona.org • Intersex Society of North America; www.isna.org The organiation founded and led by intersex people, committed to ending isolation among those born with intersex conditions and eliminating shame, secrecy and unwanted genital surgeries for people born with intersex conditions. • For a copy of the Needs Assessment “Identifying Training Needs of Health Care Providers Related to Treatment and Care of Transgendered Patients:A Qualitative Needs Assessment” contact the author, Samuel Lurie, at slurie@gmavt.net