Download
1 / 31
320 likes | 587 Views
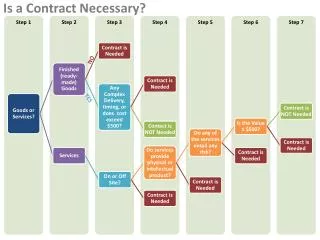
Cognitive Rehabilitation Is Medically Necessary . Kathy de Domingo, MS, CCC-SLP, Progressive Rehabilitation Associates Laurie Ehlhardt, PhD, CCC-SLP The Teaching Research Institute-Eugene. Overview of Presentation. What is cognitive rehabilitation?

E N D
Cognitive Rehabilitation Is Medically Necessary Kathy de Domingo, MS, CCC-SLP, Progressive Rehabilitation Associates Laurie Ehlhardt, PhD, CCC-SLP The Teaching Research Institute-Eugene
Overview of Presentation What is cognitive rehabilitation? Who provides cognitive rehabilitation services? Why is it medically necessary? “It’s the law!” So, what’s the problem? Toolkit (tips and tricks) for advocating for Cog. Rehab. insurance coverage
What is Cognitive Rehabilitation? • Cognitive rehabilitation is a systematically applied set of medical and therapeutic services designed to improve cognitive functioning and participation in activities that may be affected by difficulties in one or more cognitive domains. (It) is often part of comprehensive interdisciplinary programs…based upon sound scientific theoretical constructs and strategic approaches…
Cog Rehab Definition (cont) • Treatment goals vary depending on the etiology, extent and severity of injury to the brain, the timing of treatment, individual differences, phase of recovery and prospects for restoration or compensation of a problem with remedial interventions. Treatments may be process specific…or skill-based, aimed at improving performance of particular activities…
Cog Rehab Definition (cont) • The overall goal may be restoring function in a cognitive domain or set of domains or teaching compensatory strategies to overcome domain specific problems, improving performance of a specific activity, or generalizing to multiple activities.” • “Cognitive Rehabilitation: The Evidence, Funding and Case for Advocacy in Brain Injury”, BIA, Nov. 2006
Examples of Types of Cognitive Rehabilitation (CR) Executive Functions: Problem-solving & self-monitoring strategies Memory: Training use of external memory aids (ex. diaries, notebooks or PDAs) & strategies (ex. imagery) Attention: Attention process training; strategies training (ex. time management) Communication: Functional communication training (ex. listening to directions; asking for help) Task Specific Training(ex. filing tasks; dressing routines) Environmental Modifications(ex. change lighting; decrease noise)
Who provides CR services? Certified speech-language pathologists, occupational therapists, vocational rehabilitation counselors, neuropsychologists May work collectively with patients as part of a team or individually CAUTION: Some service providers claim expertise in providing these services
Why is CR medically necessary? Case example: Jill is 45 years old. TBI in a car crash. 1-year post injury; lives at home w/ husband & 2 teen-age children; former school teacher Outpatient CR services at a rehab clinic Moderate-severe cognitive-communication impairments (attention, memory, executive functions); Unsafe in several situations
Case example: Jill (continued) Not able to return to work Not safe to take her medications Can’t drive or safely walk across the street Trouble communicating wants/needs when anxious Falls when dressing herself Prone to seizures when overly-fatigued over-stimulating environments
Why is CR medically necessary? Executive functions : Easily overwhelmed when cooking and can’t self-monitor. Forgets to turn off the burners. Strategy training: Trained to use a self-monitoring strategy (“Stop-Think”).
Why is CR medically necessary? Memory: Forgets to take her medications. External memory aid: Trained to use a medication reminder box to cue when she needs to take her pills.
Why is CR medically necessary? Attention: Distracted when crossing the street; at risk for another accident Attention Process Training (APT): Improves ability to filter out distractions. Attention strategy: Trained to visually scan in both directions before crossing a street.
Why is CR medically necessary? Communication: Unable to communicate when fatigued and overwhelmed. Word finding problems. Often leads to angry outbursts and possible seizure. Functional communication training: Trained to say “I need a break.”
Why is CR medically necessary? Fall Risk: At risk for falls while dressing; unsteady on her feet. Task specific routine: Trained on a very specific way to do her dressing routine: “Step 1. lay out clothes, Step 2. sit down on edge of bed, Step 3….”
Why is CR medically necessary? General health: Prone to fatigue, headaches and sometimes seizures, particularly in noisy, brightly lit, distracting environments. Environmental modifications: She and her family only go to quiet, dimly lit restaurants. They have scheduled “quiet times” and a quiet room at home.
Medical Necessity -Example policy statement: CIGNA covers an individualized program of cognitive rehabilitation as medically necessary following a traumatic brain injury, acute brain insult, or cerebrovascular accident (CVA) when ALL of the following requirements are met: • A documented cognitive impairment with compromised functional status exists. • The individual can actively participate in the treatment plan. • Significant cognitive improvement is expected and can be demonstrated by documentation submitted on a weekly basis. • Interventions should be structured, systematic, goal directed (long- and short-term goals), individualized and restorative.
So, what’s the problem? • Not all insurance plans have paid for CR services. • Why? It’s considered: • “investigational” • “not medically necessary”
Example: Regence Blue Cross/Blue Shield • Cognitive Rehabilitation (as a distinct and definable component of the rehabilitation process) is considered investigational for all applicants, including but not limited to: • Aging population, including Alzheimer’s patients • Multiple sclerosis • Post-encaphalitic or post-encaphalopathy patients • Stroke • Traumatic brain injury • Regence Blue Cross Blue Shield policy, effective 3/1/09
Now it’s the Law! Senate Bill 381 passed in 2009: Requires health benefit plans to provide coverage for medically necessary treatment for traumatic brain injury. Adds orthotic and prosthetic devices to lists of required coverage for health care service contractors and multiple employer welfare arrangements.
Oh, but… • What we don’t know yet…. • How do insurers define “medical necessity”? • What about non-traumatic brain injuries?
Toolkit: Policy updates • When last we presented….. • Only Regence and Providence had policies of non-coverage • At least 3 had limits on the policy • Now…. • Providence reportedly offers coverage • Regence has provided clarification and will review again this year • Where we see coverage, we are noting more limits (e.g. time since injury limits)
Toolkit:How do I know if it’s covered? When verifying benefits, ask if the CPT (Current Procedural Terminology)codes associated with the service you will be provided are covered in the member’s policy If they are covered, ask if there are any associated diagnoses that would negate coverage
Toolkit:How do I know if it’s covered? • Ask for access to the company’s coverage policy. • http://blue.regence.com/trgmedpol/alliedHealth/ah20.html • http://www.aetna.com/cpb/medical/data/200_299/0214.html • Ask if there is a next step in the authorization process – sometimes the initial authorization only means that the case is being authorized for a next level review for appropriateness of services.
Toolkit:What do I do if it’s not? Inform your patient of the expectation that the services will not be covered BEFORE you provide the service. Ask the patient or their representative to give you written authorization to receive the services and assume financial responsibility in the event of non-coverage Use your appeal rights!
Toolkit:Internal Appeals/External Claims • Exhaust internal appeals process (appeal to the insurer). If denied on internal appeal, then: • Find the external claims (independent) review contact for particular state: http://www.kff.org/consumerguide/7350.cfm • Contact the Oregon Advocacy Center: 1-800-452-1694 www.oradvocacy.org • File external claims. Have supporting documents • e.g., documentation of progress, research evidence
Toolkit:Documentation Guidelines • Medically necessary • Generally relates to safety, restoration of lost function, with expectation of improvement as a result of treatment • The skills of a therapist are required to… • Conduct an evaluation to determine deficits, residual skills and plan of care • Carry out therapy services that are progressive in nature, with continual assessment of progress and barriers to improvement.
Toolkit: Documentation example • Jill X • Long term goal: Client will be modified independent in her ability to safely manage her ADL needs • Short term goal: • Client will demonstrate ability to load pill minder according to prescription and frequency at 100% accuracy. • Client use external alarms to take medications as prescribed at 100% accuracy.
Toolkit: Documentation example • Correct vs. Incorrect example. • You choose: • Client will do “Brain Train” exercises • Client will improve ability to perform tasks demanding moderately complex visual and/or auditory attention skills to 80% accuracy.
Toolkit: How to be your own advocate • Provider advocate for coverage • Documentation is your friend! • Ask questions and learn to work within the insurer’s systems.
Toolkit: How to be your own advocate • Survivor advocate for access to services • Know your insurance policy and your rights to appeal • Ask for assistance from case management • Don’t take the first “no” you hear. Ask if there are more steps available to you. • Look for external advocates • Provider you are working with • Brain Injury Association • Disability Rights Oregon
Resources • Brain Injury Association of Oregon • www.biaoregon.org • 1-800-544-5243 • Disability Rights Oregon • www.disabilityrightsoregon.org • 1-800-452-1694 • See manual with examples “Finding and using resources”