Download
1 / 1
10 likes | 145 Views
10 th RCOG international scientific congress: 5 th – 8 th June 2012 Kuching , Sarawak, Malaysia. Vaginal delivery of twins: outcomes of 503 twin pregnancies, according to parity and presentation.

E N D
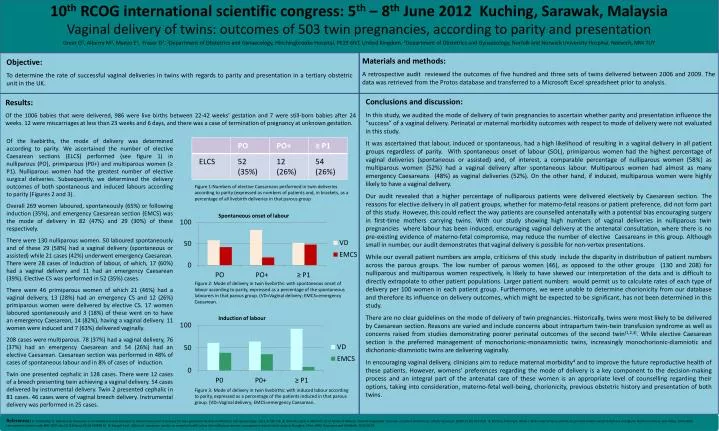
10th RCOG international scientific congress: 5th – 8th June 2012 Kuching, Sarawak, Malaysia Vaginal delivery of twins: outcomes of 503 twin pregnancies, according to parity and presentation Greer O1, AlberryM1, ManzoE1, Fraser D2. 1Department of Obstetrics and Gynaecology, Hinchingbrooke Hospital, PE29 6NT, United Kingdom. 2Department of Obstetrics and Gynaecology, Norfolk and Norwich University Hospital, Norwich, NR4 7UY Materials and methods: A retrospective audit reviewed the outcomes of five hundred and three sets of twins delivered between 2006 and 2009. The data was retrieved from the Protos database and transferred to a Microsoft Excel spreadsheet prior to analysis. Objective: To determine the rate of successful vaginal deliveries in twins with regards to parity and presentation in a tertiary obstetric unit in the UK. Conclusions and discussion: In this study, we audited the mode of delivery of twin pregnancies to ascertain whether parity and presentation influence the “success” of a vaginal delivery. Perinatal or maternal morbidity outcomes with respect to mode of delivery were not evaluated in this study. It was ascertained that labour, induced or spontaneous, had a high likelihood of resulting in a vaginal delivery in all patient groups regardless of parity. With spontaneous onset of labour (SOL), primiparous women had the highest percentage of vaginal deliveries (spontaneous or assisted) and, of interest, a comparable percentage of nulliparous women (58%) as multiparous women (52%) had a vaginal delivery after spontaneous labour. Multiparous women had almost as many emergency Caesareans (48%) as vaginal deliveries (52%). On the other hand, if induced, multiparous women were highly likely to have a vaginal delivery. Our audit revealed that a higher percentage of nulliparous patients were delivered electively by Caesarean section. The reasons for elective delivery in all patient groups, whether for materno-fetal reasons or patient preference, did not form part of this study. However, this could reflect the way patients are counselled antenatally with a potential bias encouraging surgery in first-time mothers carrying twins. With our study showing high numbers of vaginal deliveries in nulliparous twin pregnancies where labour has been induced; encouraging vaginal delivery at the antenatal consultation, where there is no pre-existing evidence of materno-fetalcompromise, may reduce the number of elective Caesareans in this group. Although small in number, our audit demonstrates that vaginal delivery is possible for non-vertex presentations. While our overall patient numbers are ample, criticisms of this study include the disparity in distribution of patient numbers across the parous groups. The low number of parous women (46), as opposed to the other groups (130 and 208) for nulliparous and multiparous women respectively, is likely to have skewed our interpretation of the data and is difficult to directly extrapolate to other patient populations. Larger patient numbers would permit us to calculate rates of each type of delivery per 100 women in each patient group. Furthermore, we were unable to determine chorionicity from our database and therefore its influence on delivery outcomes, which might be expected to be significant, has not been determined in this study. There are no clear guidelines on the mode of delivery of twin pregnancies. Historically, twins were most likely to be delivered by Caesarean section. Reasons are varied and include concerns about intrapartum twin-twin transfusion syndrome as well as concerns raised from studies demonstrating poorer perinatal outcomes of the second twin(1,2,3). While elective Caesarean section is the preferred management of monochorionic-monoamniotic twins, increasingly monochorionic-diamnioticand dichorionic-diamniotic twins are delivering vaginally. In encouraging vaginal delivery, clinicians aim to reduce maternal morbidity4and to improve the future reproductive health of these patients. However, womens’ preferences regarding the mode of delivery is a key component to the decision-making process and an integral part of the antenatal care of these women is an appropriate level of counselling regarding their options, taking into consideration, materno-fetal well-being, chorionicity, previous obstetric history and presentation of bothtwins. Results: Of the 1006 babies that were delivered, 986 were live births between 22-42 weeks’ gestation and 7 were still-born babies after 24 weeks. 12 were miscarriages at less than 23 weeks and 6 days, and there was a case of termination of pregnancy at unknown gestation. • Of the livebirths, the mode of delivery was determined according to parity. We ascertained the number of elective Caesarean sections (ELCS) performed (see figure 1) in nulliparous (PO), primiparous (P0+) and multiparous women (≥ P1). Nulliparous women had the greatest number of elective surgical deliveries. Subsequently, we determined the delivery outcomes of both spontaneous and induced labours according to parity (Figures 2 and 3). • Overall 269 women laboured, spontaneously (65%) or following induction (35%), and emergency Caesarean section (EMCS) was the mode of delivery in 82 (47%) and 29 (30%) of these respectively. • There were 130 nulliparous women. 50 laboured spontaneously and of these 29 (58%) had a vaginal delivery (spontaneous or assisted) while 21 cases (42%) underwent emergency Caesarean. There were 28 cases of induction of labour, of which, 17 (60%) had a vaginal delivery and 11 had an emergency Caesarean (39%). Elective CS was performed in 52 (35%) cases. • There were 46 primiparous women of which 21 (46%) had a vaginal delivery, 13 (28%) had an emergency CS and 12 (26%) primiparous women were delivered by elective CS. 17 women laboured spontaneously and 3 (18%) of these went on to have an emergency Caesarean, 14 (82%), having a vaginal delivery. 11 women were induced and 7 (63%) delivered vaginally. • 208 cases were multiparous. 78 (37%) had a vaginal delivery, 76 (37%) had an emergency Caesarean and 54 (26%) had an elective Caesarean. Caesarean section was performed in 48% of cases of spontaneous labour and in 8% of cases of induction. • Twin one presented cephalic in 128 cases. There were 12 cases of a breech presenting twin achieving a vaginal delivery. 54 cases delivered by instrumental delivery. Twin 2 presented cephalic in 81 cases. 46 cases were of vaginal breech delivery. Instrumental delivery was performed in 25 cases. Figure 1:Numbers of elective Caesareans performed in twin deliveries according to parity (expressed as numbers of patients and, in brackets, as a percentage of all livebirth deliveries in that parous group Spontaneous onset of labour Figure 2: Mode of delivery in twin livebirths: with spontaneous onset of labour according to parity, expressed as a percentage of the spontaneous labourers in that parous group. (VD=Vaginal delivery; EMCS=emergency Caesarean. Induction of labour Figure 3: Mode of delivery in twin livebirths: with induced labour according to parity, expressed as a percentage of the patients induced in that parous group. (VD=Vaginal delivery; EMCS=emergency Caesarean. References: 1. Christopher D, Robinson B, Peaceman A. An evidence-based approach to determining route of delivery for twin gestations. Review in Obstetrics and Gynaecology. 2011; 4:109-116 2. Little M, Lyerly A, Mitchell L et al. Mode of delivery: Toward responsible inclusion of patient preferences. ObstetGynaecol. 2008 112 (4): 913-918. 3. Smith G, Fleming K, White I. Birth order of twins and risk of perinatal death related to delivery in England, Northern Ireland, and Wales, 1994-2003: retrospective cohort study BMJ 2007;:doi:10.1136/bmj.39118.483819.554. Wang B et al.: Effects of caesarean section on maternal health in low risk nulliparous women: a prospective match cohort study in Shanghai, China. BMC Pregnancy and Childbirth. 2010 10:78